

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The first case of a bifid mandibular condyle (BMC) was presented by Hrdlička,1 who identified it in the skull specimen of a cadaver in 1941. A total of 103 cases of BMC have been reported from 1987 to 2011.2 The paucity of the reported cases indicates that BMC is an extremely unusual morphological variation. The morphological details of BMC have been reported to vary. The second condylar head has been reported to usually be located in the anterior or medial site of the original condylar head. Other cases of BMC showed variation in the depth of the groove dividing the mandibular condyle into two sections symmetrically in the sagittal plane. The extremely rare formation of a trifid mandibular condyle, with medial, central, and lateral divisions, has also been reported.3
Several authors have proposed etiologies of BMC;34567891011 but no consensus has emerged. Szentpétery et al.4 found only 7 cases of BMC in 1882 skulls (0.48%). From 2008 to 2010, Menezes et al.5 and Miloglu et al.6 found that the prevalence of BMC was 0.018% and 0.3%, respectively, using panoramic radiographs. Sahman et al.910 reported that the prevalence of BMC was 0.52% and 1.82% using panoramic radiographs and computed tomography (CT), respectively. In Cho and Jung's retrospective study using cone-beam computed tomography (CBCT),11 the prevalence of BMC was 0.5% in 7424 patients. Moreover, the female-to-male ratio ranged from 1.1 : 1 to 3.5 : 1 in these studies.35691011 Some authors47 have suggested that trauma at an early age may be a crucial factor in the development of BMC, whereas other authors368 reported no age predilection. These disagreements in statistical analyses of BMC were caused by the lack of adequate data. Furthermore, its uncertain pathogenesis and etiology make BMC a complicated subject to study.
This report describes a case of post-traumatic BMC with radiographic findings. Additionally, we summarize the pathogenic features of BMC in a review of the literature.
Case Report
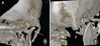
A 9-year-old female patient was referred to the Department of Oral and Maxillofacial Surgery at Sanggye Paik Hospital with complaints of pain and trismus in the right temporomandibular joint (TMJ) after a bicycle accident. Spontaneous pain in the right TMJ, mandibular deviation to the right side, restricted mouth opening, malocclusion, concussion of the upper anterior teeth, and an upper lip laceration were detected on the clinical examination (Fig. 1). A maximum jaw opening of 10 mm was achieved passively. Computed tomography (CT) showed a fracture of the right mandibular condyle (Fig. 2). Non-surgical reduction with a gunning splint was recommended while the patient remained juvenile. Circumzygomatic and circummandibular wiring were performed under general anesthesia since the patient had primary teeth, which did not allow a tooth-retaining reduction technique such as an arch bar. Active physiotherapy was conducted beginning 7 days postoperatively. A maximum jaw opening of 10 mm was obtained. The elastic intermaxillary fixation was removed, and mouth opening exercises using a tongue blade were initiated 1 month postoperatively. The gunning splint was removed and a jaw opening of 26 mm was obtained at a 2-month follow-up visit. A mouth opening of 38 mm was achieved 4 months postoperatively, and the patient was instructed to continue mouth opening exercises to achieve a normal range of motion. The patient achieved a maximum mouth opening of 45 mm at a 6-month follow-up visit and did not have any subjective symptoms. She displayed no clinical signs such as clicking sounds and tenderness of the TMJ, trismus, malocclusion, and pain; a 4-mm rightward deviation of the jaw upon protrusive movement was observed. Clinical and radiological examinations were performed regularly. A series of panoramic radiographs showed the fractured condylar head, indicating a gradual healing process (Fig. 3). At a routine 3-year routine visit after the operation, CBCT with Uni3D S (Vatech, Hwaseong, Korea) was conducted to examine the condition of the TMJ for orthodontic treatment planning. Bifidity of the condylar head was found incidentally on CBCT radiographs (Fig. 4). Another medially placed condylar head, which had been bent by the fracture, was discovered on the 3-dimensional reconstructed image (Fig. 5). The patient exhibited no clinical symptoms or signs. The jaw deviation on protrusion was also corrected.
Discussion
BMC is a unique anomaly consisting of a double-headed condyle. Its specific pathogenesis and etiology remain unknown due to its rarity. Some authors have suggested that most BMCs are asymptomatic.23568 García-González et al.12 argued that treatment is not required for an asymptomatic BMC, even if long-term follow-up is necessary due to the possibility of delayed symptoms. However, symptomatic BMCs have also been described.23471213141516 Bifid formation with a temporomandibular disorder (TMD) such as a clicking sound, restricted mandibular movement, pain, swelling, ankylosis, and facial asymmetry were noted in these studies. Antoniades et al.3 treated patients suffering from restricted jaw movement with nonsteroidal anti-inflammatory drugs, muscle relaxants, occlusal splints, and wooden tongue spatulas. García-González et al.12 also suggested that patients who had an internal derangement of the TMJ disc should receive medical treatment with splints and arthroscopic surgery. If facial asymmetry, mandibular hypoplasia, restricted mandibular movement, and other TMDs accompany a BMC with TMJ ankylosis, it should be treated surgically, through procedures such as gap arthroplasty, interpositional arthroplasty, condylectomy, and joint reconstruction.12141516
Two major causes of BMC have been suggested. The possibility that developmental factors may be involved in the development of BMC has been discussed by several authors. Blackwood17 proposed the idea of a retained well-vascularized fibrous septum embedded on the mandibular condyle in the anteroposterior direction. This septum was proposed to divide the condylar head into 2 parts mediolaterally during the developmental process. This could explain how a forceps delivery causing hematoma around the condylar head led to BMC formation.1517 Szentpétery et al.4 supported the retained septum theory, and insisted that a double-headed condyle with anteroposteriorly positioned morphology was associated with early childhood fractures, whereas those with a mediolaterally positioned morphology were caused by the persistence of a septum in the connective tissue. The growth-center theory regarding condylar head development was suggested by Antoniades et al.3 and Kahl et al.18 These researchers argued that minor trauma during puberty or childhood could result in a bifid condyle, as well as facial asymmetry, because the mandibular condyle is an important center of facial growth.3 However, Gundlach et al.19 found a BMC that did not contain fibrous septa. They induced a BMC using a teratogenic substance in a rat experiment, which caused maldirection of the muscle affecting the condylar head position. Infection, irradiation, nutritional disorders, genetic, endocrinological, and pharmacological factors have been postulated to account for this phenomenon. Cho and Jung11 suggested that developmentally originated BMCs were not associated with TMD in a retrospective study. Some authors have reported that the frequency of nontraumatic origin was much higher than that of traumatic origin.23568 The prevalence of nontraumatic BMC was reported to be 64.07% by Almasan et al.2 and 75% by Antoniades et al.3
Another important cause of BMC has been argued to be trauma related to the condylar neck or a sagittal fracture. Poswillo20 induced a BMC by condylectomy in Macaca monkeys. This study revealed that the resection site of the condylar head was able to generate a new condylar head. Hotz21 also reported formation of a new condyle in the fractured mandibular condyle of a living person. Hotz observed radiographs taken during the healing process of a fractured condylar head; an entirely new condyle had grown at the original position and the fractured condyle underwent partial resorption due to insufficient remodeling capacity. As mentioned above, Szentpétery et al.4 insisted that anteroposteriorly arranged bifid condyles must be the result of early childhood fractures. Although most reported cases of post-traumatic BMC follow the hypothesis of Szentpétery et al., Li et al.7 noted a case of BMC that was due to a sagittal fracture of the condylar head arranged in a mediolateral position.
Thorough evaluation is needed to explain these conflicting results related to the etiology of BMC. Various arguments have been adduced in favor of a developmental cause of BMC, but no consensus has emerged regarding the most likely explanation. However, it is apparent that BMC caused by developmental factors tends to form mediolaterally on the frontal plane and appears as a symmetrical form. These BMCs exhibit variation in the depth of the groove that separates the condylar head mediolaterally into 2 symmetric parts.
Post-traumatic BMC involves relatively specific factors that cause a double-headed mandibular condyle. Szentpétery et al.4 insisted that the emergence of a BMC and its symptoms were influenced by the type of injury (direct or indirect, high or low fracture), the extent of damage to the joint structures (disc, capsule, and articular surfaces), the presence or absence of inflammation, hemarthrosis, and the patient's age. Sahm and Witt22 found that a high condylar head fracture underwent high-grade remodeling, but a low condylar head fracture did not show a good remodeling result. Moreover, BMC formation occurred in some cases. Li et al.7 reported a series of 4 cases of a BMC caused by fracture, and classified the BMC appearance based on trauma severity, the fracture site, and relationship to the insertion of the lateral pterygoid muscle. Dahlström et al.23 also suggested that remodeling of the fractured condylar head was affected by the demands of function and growth. In our review of the literature, the direction of the fractured condylar head, site, severity, and its remodeling capacity were found to be the key factors involved in the formation of a BMC from the fractured state.
The lateral pterygoid muscle, which affects the direction of the fractured condylar fragment, is an important factor in BMC formation.471622 If the muscle force is adequate to dislocate the condylar head, it meets the minimum requirement for the formation of a BMC. Moreover, the ability to create a new condylar head at the original site and insufficient remodeling capacity of the fractured condylar head must occur simultaneously. It is not certain whether remodeling ability is related with age, sex, or race. The vector of the fractured condyle is also important because it regulates the arrangement of the BMC. Although Szentpétery et al.4 argued that the anteroposteriorly arranged BMC resulted from trauma, this dichotomy did not successfully explain variation in the morphology of BMCs. Rather, it seems that the arrangement of the BMC depends on the vector of the fractured condylar head and its relationship with the lateral pterygoid muscle force. Variation in BMC morphology might be also regulated by the extent of trauma. The anteroposterior groove or notch in the middle of double-headed condyle is mainly seen in sagittally (vertically) fractured or slightly deviated condylar heads. Immediately apparent Y-shaped condylar heads, however, are found in cases of severe deviation.
BMCs are difficult to detect in conventional radiographs. Most of the reported cases were found with considerable difficulty due to a lack of symptoms and the superimposition of nearby anatomic structures. A panoramic radiograph is the first choice of diagnostic tool for detecting BMC due to its easy accessibility and low cost.12 However, it has a substantial limitation because the 2-dimensional plane only allows the view to be shown on one side of the plane. Thus, mid-sagittal grooves of the condylar head were not seen on panoramic radiographs. In addition, apparent BMCs can be confused with other abnormal anatomic structures due to the presence of overlapping nearby structures or inherent radiographic distortion. Therefore, several authors have suggested that CT or CBCT is the gold-standard diagnostic tool for detecting the true prevalence of BMCs.56111618 These developments in diagnostic imagery have resulted in an increasing number of reports of BMCs in recent decades.
In this study, a young patient showed bifidity of the condylar head on the right side after a condylar neck fracture healed. The condylar head was arranged in the mediolateral position, which is the opposite of what would be expected according to the hypothesis of Szentpétery et al.4 This led us to conclude that the direction and appearance of the BMC are affected by multifactorial causes. Additionally, patients such as ours may present with no symptoms and a normal range of mouth opening with deflection to the right side. Although further investigation including more cases is needed, we speculate that BMC formation may be associated with the fracture site, deviation extent and direction, and remodeling capacity with age. The degree of symmetry of the BMC may indicate whether the origin was traumatic or developmental. A symmetric appearance usually occurs in BMCs with a developmental cause, and an asymmetric appearance is associated with a traumatic origin. In spite of these tendencies, the precise pathophysiology of BMC formation remains unresolved. Recently, advancements in imaging devices have helped to further characterize the prevalence of BMCs. Since BMC cases have been reported with increasing frequency, further study is required to ascertain the etiology of the bifidity of the condylar head.




 XML Download
XML Download