

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The practice of dentistry has seen a paradigm shift not only in the provision of quality dental care but also in the diagnosis of diseases that adversely affect the general health of a patient. With advances in medical and dental sciences, people are living longer as a result of treatment for chronic disorders, although these disorders may ultimately result in mortality. It is important for dental surgeons to be aware of a wide range of medical conditions in order to take appropriate measures in recommending medical and lifestyle modifications to improve patients' prognoses and health in general.
The key to the successful management of any patient is performing a thorough evaluation, which can help ensure the early diagnosis of any diseases the patient might have. Obstructive sleep apnea (OSA) is a common medical disorder with potentially severe health and social consequences. OSA and its associated co-morbidities12 are common medical conditions with relatively high mortality rates.3 OSA is implicated in the common complaint of simple snoring and upper airway obstruction. Untreated OSA can lead to hypertension, diabetes, cardiovascular disease and other cardiac conditions (e.g., myocardial infarction, congestive heart failure, cerebrovascular accidents, and cardiac arrhythmia), cognitive dysfunction, and depression, leading to decreased concentration and causing problems such as impairment of function and motor vehicle accidents.124
Patients at a high risk of developing OSA can be identified in a dental setting through a simple radiographic evaluation. Previous studies have assessed patients at risk of developing OSA by evaluating their clinical signs and symptoms or by measuring the airway through cephalometric analysis.5 To the best of our knowledge, no study has considered all 3 parameters (clinical examination, the Berlin questionnaire, and measurements on lateral cephalograms) as a way to evaluate patients at a high risk for sleep apnea. This study also emphasized the importance of a thorough clinical examination and the role of the Berlin questionnaire in predicting high-risk patients. The purpose of the present study was to identify patients at a relatively high risk for OSA by measuring the upper airway diameter (UAD) and mandibular-to-hyoid bone distance (MP-H) on a lateral cephalogram after a thorough clinical examination and completion of the Berlin questionnaire.
Materials and Methods
After obtaining institutional ethical clearance (IRD: PMVIDS&RC/ IEC/ OMR/ PR/ 0049-15), we conducted a study on patients visiting our dental hospital for routine dental problems. A comparative cross-sectional study was done on male and female patients>18 years of age who received care in our dental outpatient department.
Patients>18 years of age were included in the study, since it has been reported that the size of the nasopharynx is closely correlated with skeletal growth, age, and the developmental changes that occur in the pharyngeal airway from childhood to young adulthood. All patients were thoroughly examined for clinical features such as craniofacial abnormalities, a deviated nasal septum, macroglossia, tonsillar hypertrophy, large neck circumference, and malocclusion, and were asked about the presence of risk factors such as diabetes mellitus and coronary artery disease. Patients with one or more of the above mentioned criteria were included in the study. Patients not willing to participate in the study and patients<18 years of age who had already been diagnosed with OSA were excluded from the study.
All patients were given the Berlin questionnaire,4 a validated instrument comprising 10 questions in 3 categories (snoring, daytime drowsiness, and hypertension/obesity). In Category 1, high risk was defined as persistent symptoms reported in response to 2 or more questions about snoring. Category 2 measured daytime sleepiness and drowsy driving, with persistent occurrence classified as high risk. The presence of hypertension or obesity was determined in Category 3. Patients positive for 2 or more categories in the questionnaire were considered to be in the high-risk group (OSA group); patients positive for 1 category or for no categories were assigned to the control group.
All patients in the high-risk and control groups underwent a digital lateral cephalogram using a Planmeca Proline XC machine (Planmeca Oy, Helsinki, Finland). The UAD was measured from the point on the anterior half of the soft palate to the closest point on the outer pharyngeal wall.11 The MP-H was measured by drawing a tangent to the mandibular plane, then measuring the distance to the hyoid bone from that tangent (Fig. 1). Both measurements were made by 2 observers at 2 different times with a gap of 10 days to avoid bias caused by interobserver and intraobserver variability.
The data were statistically analyzed by the Student's unpaired t test using SPSS version 18 (IBM, Chicago, IL, USA). P-values<0.05 was considered indicative of statistical significance. The mean, standard deviation, and standard error of the mean were calculated. The UAD and MP-H were compared between the OSA and control groups, and between males and females. The patients were divided into 5 age groups (18-25, 26-35, 36-45, 46-55, and 56-65 years); the UAD and MP-H were compared among the different age groups to determine whether age had a significant relationship with the outcomes. The Student's paired t test was performed to assess intraobserver and interobserver variation.
Results
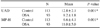
In the sample of 206 patients, 93 (45%) were in the OSA group (the high-risk group) and 113 (55%) were in the control group based on the results of the Berlin questionnaire. The sample comprised 91 males and 115 females. All patients ranged in age from 18 to 65 years. The mean UAD in the OSA group was 8.2±1.8 mm and 12.8±2.1 mm in the control group; the MP-H was 11.0±5.0 mm and 6.6±4.1 mm in the OSA and control groups, respectively. The UAD measurements in the OSA group were significantly lower than in the control group, and the MP-H in the OSA group was significantly greater than in the control group (P=0.001) (Table 1).
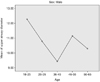
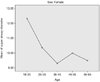
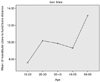
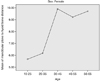
The UAD measurement was calculated in the different age groups among males and females, and significantly lower values were found in middle-aged males and females (age range, 35-46 years) (Figs. 2 and 3). The MP-H measurement was also calculated in the different age groups among males and females, and significantly greater MP-H values were found in older men (age range, 56-65 years) and middle-aged women (age range, 36-45 years) (Figs. 4 and 5).
The MP-H was compared between males and females to determine whether any significant difference was present in this parameter according to sex. The MP-H measurements were significantly greater in males than in females, whereas the UAD measurements showed no significant difference according to sex (Table 2).
Discussion
OSA may be caused by several factors that lead to upper airway collapse. Thorough clinical examination and risk factor analysis aid in identifying patients who are at a high risk for developing sleep apnea. In our study, of the 206 patients given the Berlin questionnaire, 45% were in the high-risk group and 55% were in the control group. The fact that participants were classified based on the Berlin questionnaire scores highlights the importance of a thorough clinical examination and risk factor analysis. This is in accordance with studies of OSA in patients with tonsillar hypertrophy,6 macroglossia,7 and craniofacial abnormalities. 8
Our results showed significantly lower UAD values in the OSA group than in the control group. Researchers have previously reported smaller airway diameters in patients with OSA.910 Szymanska et al.11 reported smaller upper airway diameters than the standards set by Mc-Namara on lateral cephalograms in patients with OSA. Martin et al.12 found that as the upper airway diameter decreased, the number of apnea or hypopnea episodes increased. They also concluded that these values decreased even more sharply if patients were examined while lying down.
We found a significantly higher value of the MP-H in the OSA group (11.0 mm) than in the control group (6.6 mm), suggesting that an inferiorly placed hyoid bone is present in patients at a relatively high risk for OSA. In a meta-analysis by Armalaite et al.,5 the MP-H distance was 4.14 mm greater in OSA patients than in the controls. They concluded that higher MP-H values might serve as a predictor for differentiating normal subjects and patients with OSA.
We found that middle-aged men and women showed significantly lower UAD values (age range, 35-46 years). This could be attributed to age being a predisposing factors for OSA.4 We also found significantly higher MP-H values in the older age group in men (56-65 years) and middle-aged women (36-45 years). Gabbay and Lavie13 concluded that OSA severity varied with age in both genders, and that women had less severe manifestations of the condition across all age categories. Obesity, snoring, hypertension, and excessive daytime sleepiness were OSA predictors in both genders, while insomnia-related complaints were negative predictors.
Men had a significantly more inferiorly placed hyoid bone in both the OSA group and the control group in our study. In a similar study by Guttal et al.,14 the hyoid bone was found to be more inferiorly placed in males than in females. Block et al.15 studied 30 asymptomatic men and 19 asymptomatic women who were monitored during one night's sleep to determine the incidence of breathing abnormalities and oxygen desaturation in normal subjects. The sex differences were highly significant with male predominance.
Julià-Serdà et al.16 noted that cephalometry combined with clinical variables, physical examination, and nocturnal oximetry were useful in the diagnosis of OSA, and suggested that the use of these methods can significantly reduce the number of polysomnography studies undergone by patients. The present study further emphasizes the importance of clinical signs and symptoms by combining the Berlin questionnaire with assessment of the UAD and MP-H to identify patients at a high risk of developing sleep apnea.
In conclusion, cephalometry was found to be a useful modality for assessing the UAD and MP-H. Cephalometry cannot be used for assessing the transverse diameter, but it may be a promising tool for predicting patients at a high risk of sleep apnea. We concluded that UAD values were significantly lower and MP-H values were significantly higher in patients at a high risk of developing OSA as assessed by the Berlin questionnaire in comparison to other patients. OSA can pose a great risk to individuals and is associated with a high morbidity rate. Simple measures to assess patients at a high risk of OSA may play a vital role in early diagnosis, which can significantly improve patients' prognoses.




 XML Download
XML Download