

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Clinicians are increasingly utilizing Cone-Beam Computed Tomography (CBCT) is in the field of dentistry for various diagnostic tasks.12 It provides volumetric information, orthogonal reconstruction, and cross-sectional image data.3 Reconstructed orthogonal images provide geometrically concordant linear measurements which is not possible with conventional 2D imaging.34 CBCT scans can be obtained with different fields of view (FOVs).2 CBCT scans typically cover a larger FOV and capture not only the dentoalveolar region, but also the extragnathic region.2 This leads to the possibility of identifying incidental findings outside the region of interest, such findings may sometimes be overlooked by untrained eye.267 Previous data from literature suggests that approximately 25% of CBCT images obtained for various maxillofacial diagnostic tasks displayed incidental findings.68
The clivus is a very important part of the skull base and is usually captured in large FOV scans. The clivus may be associated with multiple anatomical variations and pathologies, such as canalis basilaris medianus (CBM), chordoma etc. CBM is an uncommon anatomical variant of the basiocciput.9 Jacquemin et al.9 stated that Gruber was the first to describe about CBM. Clinically asymptomatic, it is a congenital defect that has been observed in approximately 2% of dry skulls.910 CBM has been broadly classified into complete or incomplete channel types.9 Two theories have been proposed regarding the origin of this transclivial defect. One is vascular theory and another one is notochordal theory. Vascular theory states that it could have originated from emissary vein. Notochord theory predicates that this defect could be reminiscent part of notochord. 910 Previous studies have evaluated CBM using dry skulls, computed tomography (CT) and magnetic resonance imaging (MRI).910
This report describes two presumed cases of CBM detected utilizing the CBCT imaging modality along with a review of the literature. To the best our knowledge, this is the first case series to be reported using CBCT imaging.
Case Report
Case 1
The CBCT data of a 11-year-old female was referred to evaluate radiolucency in the apical area of the maxillary left lateral incisor. The patient presented with no clinical symptoms and had a non-contributory medical history. The CBCT scan was obtained with i-CAT unit (Imaging Science, Hatfield, PA, USA). The Digital Imaging and Communications in Medicine (DICOM) deidentified data was sent through a Health Insurance Portability and Accountability Act-compliant secure email (Brightsquid, Ross Technology Centre, Calgary, Alberta, Canada) and the data was evaluated using InVivo5.4.3 (Anatomage, San Jose, CA, USA).
All data was evaluated by two board-certified oral and maxillofacial radiologists (SAZ, SAR). The orthogonal views of the large FOV revealed an incidental finding in the clivus. It was observed that the sagittal view was optimal for the visualization of this entity because of its extension in the anterioposterior direction across the clivus. Radiographically CBM can be described as a well-defined, corticated and channel-like hypodense radiolucency extending from the pharyngeal aspect of the basiocciput to the intracranial aspect of the clivus. This radiographic presentation is pathognomonic representation of CBM. No other advanced imaging was advised since the patient was asymptomatic (Fig. 1).
Case 2
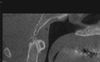
A 63-year-old female patient with a significant medical history of arthritis, thyroid disease, sinusitis, and gastrointestinal disease was referred for a CBCT scan. The volumetric scan was acquired via a CS9300 machine (Carestream Inc., Atlanta, GA, USA), and the patient was referred for the evaluation of a proposed implant site in the maxillary region. The data was analyzed using multiplanar reformatted slices by a board-certified oral and maxillofacial radiologist (MM). The volumetric data set revealed an unusual finding on the basiocciput of the clivus. In the sagittal view the intracranial part of the clivus showed discontinuity, the radiographic presentation of this osseous defect presentation can be described as a well-corticated, hypodense channel extending in the superior-inferior direction along the intracranial aspect of the clivus (Fig. 2). On initial inspection it appeared to be a fracture of the clivus. However, further close inspection revealed no other signs of osteolytic destruction on the posterior aspect of the clivus (intracranial surface). Based on the volumetric appearance of the defect, a radiographic impression of CBM was made. This transclival defect can be best appreciated on the sagittal view. This entity depicted is an example of the complete type of CBM.
Discussion
The term CBM is used to describe transclival defect of the basicocciput of the clivus. CBM presents itself in various configurations such as keyhole defect, transverse or longitudinally fissures in the clivus.12 Radiological features of CBM can be described as a well-defined, corticated, osseous transclival defect located in the basiocciput of the clivus. In the axial view it is located in close approximation to the anterior rim of the foramen magnum.10 CBM's reported prevalence in the literature is is 2%-3% for adults and 4%-5% in children.910
Six varieties of CBM (Fig. 3) were described in the literature: three complete varieties (superior, inferior, and bifurcated) and three incomplete varieties (a thin, long channel; and either a superior recess; or an inferior recess).910 The complete type of CBM is characterized by the presence of a channel or tract like hypodense region extending either anterio-posteriorly or superior-inferior direction occasionally, connecting the intracranial and pharyngeal portions of the clivus. Incomplete type will traverse partially within the clivus and they fail to communicate with pharyngeal portion or intracranial of the portion of the clivus.
CBM in general is considered an anatomical variant without any clinical significance.89 However, few studies indicate that they could serve as potential pathways for the progression of the disease such as meningitis.13 Hemphill et al.11 and Martinez et al.12 reported a transclival bony defect that was associated with a meningocele and caused recurrent meningitis.
Jacquemin et al.9 presented a case of the incomplete inferior type of CBM. The osseous defect was located at the level of pharyngeal fossa. Their patient presented with atypical bacterial meningitis. However, authors argued that a mere coexistence of CBM and meningitis may not have caused detrimental effects such as optic neuropathy and the episode of sterile meningitis as noted in their case.9
Lohman et al.13 reported a CBM in association with a Tornwaldt cyst for the first time in the literature. Their case demonstrated the potential overlap of these entities.
Literature is providing conflicting reports about CBM's association with other pathological entities such as meningitis, Tornwaldt's cyst and its detrimental effects as noted in the above description. Further future studies are recommended to find its association with other pathological entities.
We reported two cases of CBM. First case described was incomplete type and second case was complete type of CBM, both cases were assessed using CBCT. In both the cases, the occurrence of CBM was not associated with meningitis or other problems. Our experience, as well as the literature as a whole, emphasizes the need for thorough analysis of skulls regardless of whether defects are detected or not when diagnostic tools such as CBCT, CT, and MRI are readily available.25 We recommend that all data should be interpreted by a board-certified oral and maxillofacial radiologist to prevent misdiagnoses and to avoid potential complications.7


 XML Download
XML Download