

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intraoral digital radiography has been used widely in the field of dentistry. The use of this imaging method may improve the diagnosis of carious lesions. Digital imaging modalities eliminate chemical processing and hazardous waste materials. Further, the obtained images can be electronically transferred to other healthcare providers without any alteration of the original image quality.1
A photostimulable phosphor (PSP) system has been reported to be comparable with three different charge-coupled device (CCD) systems2 and conventional film3 in the detection of approximal caries. All processes that can increase the quality of, save, or in some way, modify digital images are recognized as acceptable processing operations. Different image processing methods such as contrast and brightness adjustment, histogram equalization, and noise reduction have been evaluated in various studies.4567 Image enhancement serves as a tool that modifies and improves the original version of an image. Increasing contrast, adjusting brightness, and reducing unsharpness and noise can improve subjective enhancement. Møystad et al.4 revealed that enhanced storage phosphor images compared with unenhanced images improved the detection of approximal caries.
Magnification is another option in digital software that can be adjusted. Haak et al.8 have shown that the magnification of images on a cathode ray tube (CRT) monitor may significantly influence the observer's ability to accurately detect approximal caries; further, they have asserted that the image size ratios of 1 : 1 and 1 : 2 produced higher diagnostic validity than any other ratio.
In different maxillofacial radiology clinics, various processing methods of intraoral radiographs are used for the detection of radiographic details. However, there is no standard method of image processing that has been accepted to improve caries diagnosis, and this is a common challenge for researchers and dentists. Thus, in view of the value that radiological detection of non-cavitated proximal caries has and the potential ability to manipulate digital radiographs so as to improve the quality of images, the aim of this study was to assess the influence of the changes that different variables such as sharpness and enhancement with or without magnification have on the accuracy of digital PSP systems in the detection of carious lesions.
Materials and Methods
This in vitro study was performed on 48 posterior teeth (96 proximal contacts) that had been extracted during orthodontic or periodontologic treatment with caries-free or carious proximal surfaces; this set of teeth included 24 premolars and 24 molars. Recurrent caries were artificially built in a number of teeth (19 surfaces) by leaving caries therein following cavity preparation or by applying a wax layer (thickness: approximately 1 mm) on the remaining caries undergoing restoration. The teeth were set in six different plaster models to reconstruct anatomical proximal contacts. Each pair of these plaster models of the upper and lower jaws occluded each other.
Then, six bitewing radiographs were taken using a PSP sensor (Digora, Soredex, Helsinki, Finland) having exposure parameters of 70 kVp, 7 mA, and 0.16 s, and subsequently, exposed by a Miniray intraoral X-ray unit (Soredex, Helsinki, Finland). A bitewing film holder (Kerr Hawe SA, Bioggio, Switzerland) was used for sensor positioning (Fig. 1). The image files were scanned with a Digora Optime image reader device (Digora, Helsinki, Finland) and were processed using Scanora version 0.8 software (Digora, Helsinki, Finland) in six digital processing steps and later saved as JPG images.
All originally captured images were processed using a six-step method as follows: (1) applying the "Sharpening 2" and one-time "Noise Reduction" processing options to the original images (Figs. 2A and B); (2) applying the "Magnification 1:3" option to the image obtained in the first step; (3) enhancing the original image by using the "Diagonal/" option (Fig. 3A); (4) reviewing the changes brought about by the third step of image processing and then applying "Magnification 1:3" to the image obtained in the third step (Figs. 3A and B); (5) applying the "Sharpening UM" option to the original image; and (6) analyzing the changes brought about by the fifth step of image processing, and finally, applying "Magnification 1:3" to the image obtained in the fifth step. The images processed in each step were saved in separate folders.
It should be noted that "Sharpening 2," "Noise Reduction," "Diagonal/," and "Sharpening UM" are processing functions in the Scanora 0.8 software. For example, "Sharpening" induces the sharpening of the original image and has values ranging from 1 to 4 with the highest value designated as "Sharpening UM" (Fig. 4).
The three observers, who are specialists in the field of operative dentistry with over four years of experience each, reviewed and evaluated the resulting images after a mean interval of three days on a 17-inch monitor (Dell, Round Rock, TX, USA). The observers had unlimited viewing time and recorded their opinions concerning the presence or absence of decay, on specially designed forms by using a four-point scoring system (1. definitely not caries; 2. probably not caries; 3. probably caries; 4. definitely caries). During the statistical analysis, observer scores of 1 and 2 signified the absence of caries (0) and the scores of 3 and 4 indicated the presence of caries (1). The detected dental caries were classified and numbered as (1) enamel, (2) dentine, or (3) recurrent.
After the images were viewed, the teeth were subsequently sectioned for a histological analysis to serve as the gold standard for radiographic examination by using a generic metal disc and a micromotor handpiece rotor M45 (Marathon, Henan, China) at a speed of 35,000 rpm; the disc and the rotor were perpendicular to the occlusal surface in the mesiodistal dimension.
The samples were then examined using a stereomicroscope (Olympus SZ X12, Tokyo, Japan) that had a magnification power of 8× to 50×. In this study, the data were transferred to IBM SPSS Statistics for Windows version 19 software (IBM Corp., Armonk, NY, USA) for statistical analysis. A chi-squared test was used to determine and compare the diagnostic accuracy level of the three observers. Diagnostic accuracy indices including sensitivity, specificity, and positive and negative predictive values were determined. Cohen's kappa test was used to determine the observer agreement. Statistical significance was considered to be less than 0.05 (p<0.05).
Results
This in vitro study was performed on 96 proximal contacts of 48 extracted teeth to evaluate the effects of a six-step digital processing method on the diagnostic accuracy of detecting non-cavitated proximal caries on PSP images.
The results of the microscopic evaluation revealed that 69.8% of the sample contact points had dental caries. Enamel, dentine, and recurrent carious lesions were reported at a frequency of 29.85%, 46.27%, and 23.88%, respectively.
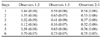
The observers' diagnostic accuracy as observed during the six different processing steps is presented in Table 1. The lowest and highest diagnostic accuracy levels were reported at the fourth and the sixth steps. The overall accuracy level was determined to be 41.7% on the basis of the 576 proximal contact reports filed by the three observers. The accuracy levels of these three observers ranged from fairly weak (18.8) to intermediate (54.2) at various steps, and the differences were deemed to be statistically significant (p=0.0001). As shown in Table 1, Step 4 was the only step in which a statistically significant difference was determined compared to all the other steps (p<0.05).
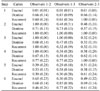
As presented in Table 2, the sensitivity, specificity, positive predictive, and negative predictive values were higher for Observers 1 and 2 at the sixth step.
Kappa values were divided into six categories according to the level of observer agreement (Table 3). According to Cohen's kappa test (Table 4), the high levels of agreement were noted between Observers 1 and 2 and between Observers 1 and 3 at the sixth step (that is, kappa values of 0.70 and 0.73, respectively). The highest agreement was obtained between Observers 2 and 3 at the fifth step (kappa value=0.76). The agreement level as determined by the corresponding kappa value was deemed good at the sixth step for all observers.
However, according to de Paola and Alman,9 the percentage agreement level tends to be higher when a caries-free surface is included in the calculation of a specific agreement level. Thus, in our study, the consistency ratio (CR) was used. According to Table 5, the rate of agreement was the highest between each pair of observers at Step 6 for the detection of caries. The agreement level of our three observers with respect to the detection of the various types of dental caries is shown in Table 6. Overall, the inter-observer agreement at Step 2 for all types of caries was higher than at the other steps of PSP image processing.
Discussion
Radiography is a standard diagnostic tool used for the evaluation of approximal caries that are not readily visible by dental practitioners. Digital radiography is a relatively new diagnostic method; recently, this method has been used increasingly in dental clinics.
Radiography and clinical findings are considered to be routine diagnostic tools in the diagnosis of approximal caries. Unfortunately, currently, there is no relatively sensitive or precise method available for the early detection of caries. Detection of a non-cavitated lesion in the early stage is crucial for preventing the progression of the carious lesion and for preserving the tooth structure through conservative but not restorative treatment.101112
In a study by Syriopoulos et al. on the radiographic detection of approximal caries by comparing dental films with digital systems, the ability of dentists to recognize caries, and not the imaging modality, was the main variable.13 Therefore, in our investigation, we used three observers who had both the same specialty and more than four years of experience of caries detection. By imposing these criteria, we could reduce observer variation in the detection. Hintz et al. have suggested that stereomicroscopy is the most reliable method to validate various studies on the accuracy of caries detection.14 Therefore, evaluation of sectioned teeth by stereomicroscopy is recommended to ensure the accuracy of caries detection.
Møystad et al. have compared X-ray films with enhanced and unenhanced storage phosphor images and have shown that the enhancement of PSP images improved the detection of approximal caries.4 An additional study on the effect of image magnification on the diagnostic accuracy of approximal caries has also revealed that magnified PSP images had a higher diagnostic accuracy level than the unmagnified form.3
In the present study, the overall diagnostic accuracy level of approximal caries was 41.7%, ranging from weak to intermediate. In fact, the application of different digital processing methods did not increase the diagnostic accuracy. The reasons for this finding could be related to the various factors that will be discussed herein. It seems that the selection of the type of digital processing method to use is somewhat individualized. In this study, the observers were only allowed to observe radiographs after applying different processing steps. Our observers had notably more experience in assessing conventional radiographs than in evaluating PSP images. Accordingly, the observers primarily used a combination of radiographic and clinical findings even though the use of only radiographic images would have been effective in the detection of caries. Another reason for the decreased diagnostic accuracy is that the actual depth of a carious lesion is often deeper than that seen radiographically, and this is attributed to the fact that carious lesions confined to the enamel may not be obvious until about 30%-40% demineralization has occurred.15
Histological examination of the 96 dental surfaces showed that 30.2% of the surfaces were non-carious. However, of the surfaces of carious lesions, 29.85% were confined to the enamel, 46.27% extended into the dentinoenamel junction (DEJ) and the dentine, and 23.88% were classified as recurrent caries. According to Abesi et al.16 and Seneadza et al.,17 diagnostic accuracy is related to the depth of the carious lesion. In our study, nearly 30% of the carious lesions were enamel caries, which could have influenced the diagnostic accuracy level, and because these carious lesions were not sufficiently deep, the diagnostic accuracy decreased. The Yoshiura study has shown that perception plays an important role in the diagnosis of approximal caries, and therefore, the diagnostic accuracy is correlated with the psychophysical properties of the imaging system,18 thus implying that an improvement in the quality of the physical image leads to increased diagnostic performance.
The highest diagnostic accuracy level for proximal caries detection was obtained at Step 6 and the second highest at Step 5. Therefore, the application of the "Sharpening UM" and "Magnification 1:3" processing options improved the accuracy of caries detection. The lowest accuracy level was achieved at Step 4 and the second lowest at Step 3. This indicates that the application of the "Diagonal/" enhancement and "Magnification 1:3" image processing options had a lesser effect on the accuracy level of caries detection.
Most of the magnified digital images processed at Steps 2 (47.9%) and 6 (54.2%) had significantly higher accuracy levels than those in the unmagnified state at Steps 1 (42.7%) and 5 (51%). These findings are similar to the results obtained by Svanaes et al.3 Therefore, our study has shown that the 1:3 magnification of digital images can influence observer performance in the detection of approximal caries.
Overall, diagnostic accuracy indices including the sensitivity, specificity, and positive and negative predictive values reveal the highest rank at Step 6 for Observers 1 and 2 and the second highest at Steps 5 and 6 for Observer 3. A noteworthy point is that the changes in image quality at Step 6 increased the diagnostic accuracy level of all observers, and this step was the common point of agreement for them. Thus, the application of the "Sharpening UM" and "Magnification 1:3" processing options increased the levels of observer accuracy in the detection of approximal caries.
According to the inter-observer agreement based on kappa values, the observer agreement in the evaluation of approximal caries was good at Steps 5 and 6. However, the agreement levels of each pair of observers based on the type of caries revealed that at Step 2, the agreement in the detection of enamel and recurrent caries was higher than at other steps and with respect to dentine caries, was dominant at Step 6. The agreement of observers in the diagnosis of dentine caries was moderate to good and that in the detection of recurrent caries was moderate to excellent. Therefore, various image enhancements and the phenomena of digital processing could compensate for the low resolution of digital imaging to accurately diagnose caries.
In the determination of the observer agreement level, intact surfaces were also included, which led to an increased agreement level. Thus, for solving this problem, a CR that focused only on carious surfaces was used. In our study, the highest CR (%) of the inter-observer agreement was reported to range from 0.70 to 0.75 at Step 6.
In the investigative study by Naitho et al. on the observer agreement in the detection of proximal caries with direct digital intraoral radiography, observers were permitted to change display settings such as brightness and contrast in a dark room. The overall kappa value in their study was moderate (0.439).19 In our study, the inter-observer agreement levels in different steps ranged from moderate to good.
In summary, our findings show that the application of "Sharpening UM" with the "Magnification 1:3" processing option improved diagnostic accuracy and observer agreement as opposed to other image processing procedures.








 XML Download
XML Download