

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In endodontic treatment, understanding the internal anatomy of the root and the root canal system plays a decisive role in the success of treatment.1 For this reason, these topics have long been a focus of active research.
Two frequent anatomical variations are found in the mandibular molars: distolingual (DL) roots of the mandibular first molar and C-shaped canals of the mandibular second molar. The typical morphology of the mandibular first molar involves two distinct roots, and the most common variation is the presence of an additional DL root.2 The DL root of the mandibular first molar was first reported in 1844, and was named the radix entomolaris.3 The prevalence of DL roots of the mandibular first molar among Caucasians is 0.7%-4.2%.245 In contrast, the prevalence of DL roots among East Asians has been reported to be 5%-40% or higher.678 Therefore, DL roots are regarded as a normal morphologic variation among East Asians.
DL roots of the mandibular molars are not simply a branch of the distal root, but an additional true root with a separate root canal orifice and a separate apex.9 Its morphology varies, from a pattern involving short conical extension to the presence of a mature root with a normal length and a root canal.49 In general, DL roots of mandibular molars have been found to be smaller and more curved than other roots, with a tendency to have a more buccally oriented apical area.2451011 A C-shaped canal is likewise a frequent anatomical variation in the mandibular second molar in East Asians.12 Although DL roots of the mandibular first molar and C-shaped canals of the mandibular second molar are two major morphologic variations in East Asians, no reports have assessed their concurrent appearance.
This study aimed to evaluate the prevalence of DL roots in mandibular molars and to analyze the root canal system of DL roots. In addition, the concurrent appearance of a DL root in the mandibular first molar and a C-shaped canal in the mandibular second molar was investigated.
Go to : 
Materials and Methods
The protocol of this study was approved by the Institutional Review Board of Wonkwang Dental University Daejeon Hospital. Cone-beam computed tomographic (CBCT) images obtained between January 2012 and December 2012 contained in the records of Wonkwang University Daejeon Dental Hospital were screened and examined. CT scans were taken using Alphard VEGA scanners (Asahi Roentgen, Kyoto, Japan) without taking the clinical objectives into account. The following settings were used: field of view, 512×512 mm; 80 kV; 5.00 mA; exposure time, 17 s; voxel size, 0.39 mm; and slice thickness, 1.00 mm.
Personal details, including the sex and age of the subjects, were also recorded. Out of 1056 mandibular molars from 264 patients, teeth satisfying the following inclusion criteria were selected for analysis: 1) mandibular molars should be fully erupted on both sides; 2) the age of patients should be over 15 to ensure complete root formation; 3) mandibular molars should not show any obvious carious lesions, root canal filling, or restorative filling of the pulp chamber space.
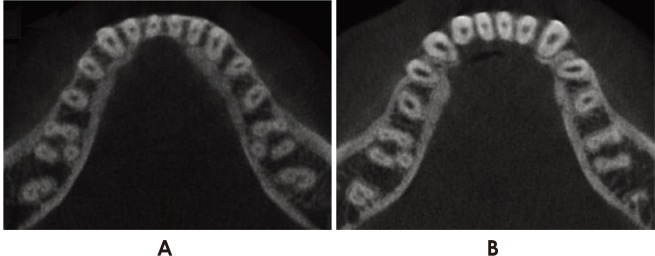
Digital Imaging and Communications in Medicine (DICOM) images with a 1-mm slice thickness were imported and prepared using the Asahivision software (Asahi Roentgen Co., Nagoya, Japan). The images were analyzed by two investigators in two sessions, with a one-month interval between the sessions. Teeth were classified as having a DL root if the DL root was clearly visible on serial axial CBCT images (Fig. 1).
The entire length of the DL root was measured as the linear distance between the cemento-enamel junction and the root apex. In the axial slice at the level of the cementoenamel junction, the center points of the distobuccal (DB) and DL canals were marked. The measurement module of the Asahivision software was then used to measure the interorifice distance, which was defined as the distance between those two points.
In order to measure the curvature, an imaginary center of the DL root canal space was created in each image slice using all three planes. The Asahivision software automatically displayed the location of the designated points as three-dimensional (3D) coordinates (x, y, and z) (Fig. 2A). The x-axis (left/right axis) was parallel to the frontozygomatic (FZ) line. The y-axis (posterior/anterior axis) was perpendicular to the FZ line and parallel to the Frankfort horizontal (FH) line. The z-axis (vertical axis) was perpendicular to both the FZ line and the FH line. The 3D coordinates (x, y, and z) of each landmark represented its 3D position relative to the origin.
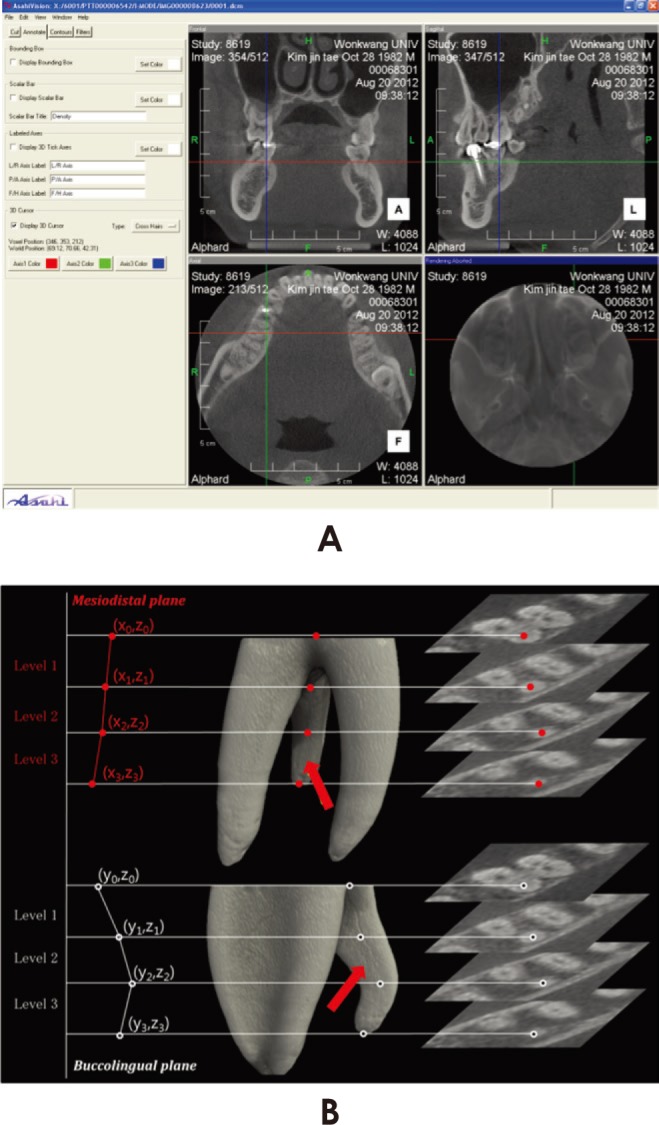 | Fig. 2A. Cone-beam computed tomographic images are displayed in three planes. The software automatically displays the locations of the designated points using three-dimensional coordinates (x, y, and z). B. The schema for the current study design. Red arrows indicate the distolingual roots of the mandibular molars. The centers of the root canals are plotted manually, and individual points are connected to create curves.
|
The center of the DL root canal of every slice between the starting point (x0, y0, and z0) and the designation point (xn, yn, and zn) was plotted manually. The line connecting the individual points then formed the axis of the canal along the curve of the root canal. The section between the starting point and the point in the next slice was set as level 1, with larger level numbers therefore indicating a location closer to the apex (Fig. 2B).
The slope of a line connecting two adjacent points indicated the root canal curvature at a given level. This was calculated using Microsoft Office Excel 2010 (Microsoft Corp, Redmond, WA, USA). In order to compare the DL root canal curvature between the buccolingual (BL) orientation and the mesiodistal (MD) orientation, separate calculations were performed using the x-components and y-components.
The DL root was then divided into coronal, middle, and apical thirds, and the curvatures for the individual thirds were calculated using the method described above. The levels corresponding to the maximum curvature values in the BL and the MD orientation were analyzed.
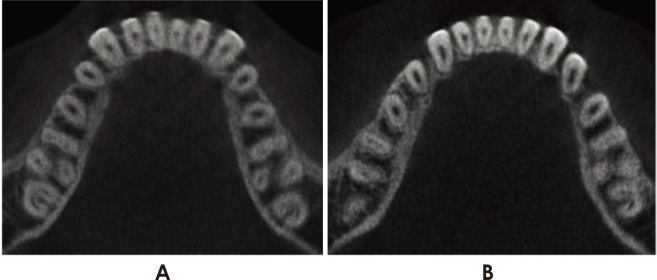
The records of patients in whom a DL root was observed in the mandibular first molar were examined to determine whether the patient also had a C-shaped canal in the mandibular second molar (Fig. 3).
The prevalence of DL roots was calculated, and Pearson's chi-square test was used to determine whether they exhibited a statistically significant tendency to occur on either the right or the left side. The occurrence of DL roots of the mandibular molar according to sex was also analyzed using the Pearson chi-square test. The paired t-test was used to compare DL root canal curvature between the BL orientation and the MD orientation. Pearson's chisquare test was used to determine whether a statistically significant relationship existed between the occurrence of a DL root in the mandibular first molar and the occurrence of a C-shaped canal in the mandibular second molar. All statistical tests were set at the 95% confidence level (p<0.05) using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Go to :
Results
In 1056 mandibular molars from 264 patients (136 males and 128 females), 105 DL roots were observed in mandibular first molars, whereas only three were found in mandibular second molars. DL roots in the mandibular molars were observed in 69 patients (26.1%). The prevalence of DL roots in mandibular first molars was found to be 20.1%. Bilateral DL roots were observed in 39 patients. Of those in whom a unilateral DL root was observed, 36.7% of subjects (11/30) had the DL root on the left side, whereas 63.3% (19/30) exhibited a DL root on the right side. The subjects ranged in age from 15 to 45 years (mean age, 25.4 years). The prevalence of DL roots was 27.2% (37/136) among males, and 25.0% (32/128) among females, which was not a statistically significant difference. Of the 1056 mandibular molars examined, the three cases where a DL root was found in the mandibular second molar were all unilateral. In two of these three cases, a DL root was also observed in the mandibular first molar.
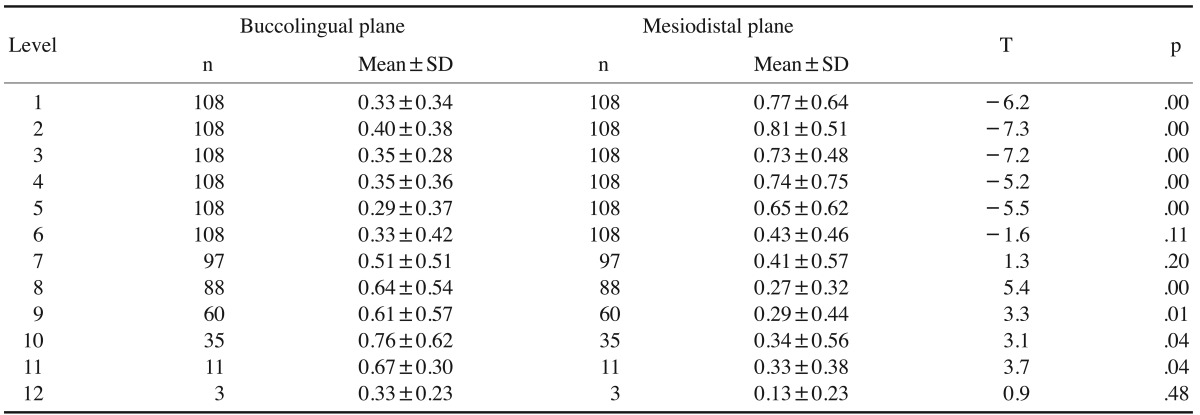
The mean length of the 109 DL roots was 8.6±1.6 mm, as assessed using four to 12 slice images. The mean interorifice distance between the DL canal and DB canal was found to be 2.8±0.2 mm. A comparison of the curvature between the BL orientation and the MD orientation showed that the change of slope in the MD orientation was larger in levels 1 through 5 (p<0.05); but in levels 8 through 11, the change of slope in the BL orientation was larger (p<0.05). No significant differences were found at levels 6, 7, and 12 (Table 1).
When roots were trisected into coronal, middle, and apical thirds, the maximum canal curvature was observed most frequently in the apical third in roots with a BL orientation, whereas maximum canal curvature was most frequently observed in the coronal third of roots with a MD orientation (Table 2).

Sixty-nine patients in whom a DL root was observed in the mandibular first molar were evaluated to determine if they also had a C-shaped canal in the mandibular second molar. A C-shaped canal was observed in 26 of the mandibular second molars (37.7%) in such subjects. C-shaped canals were bilateral in 80.8% of cases where they occurred together with a DL root in the mandibular first molar.
Go to :
Discussion
In this study, the prevalence of DL roots in the mandibular molars was investigated using CBCT images, and the general anatomy and root canal curvature were analyzed using a 3D coordinate system. A high prevalence of DL roots in mandibular molars was found among Koreans, in agreement with the results of previous studies.13141516
DL roots can occur in the mandibular first molar, mandibular second molar, and mandibular third molar, although they appear most frequently in the mandibular first molar and rarely in the mandibular second molar.517 The few reports that have evaluated the presence of DL roots in the mandibular second molar found a prevalence of 0.7% among Koreans13 and 0.38% among Japanese.18 In the present study, the prevalence of DL roots in the mandibular second molar was 0.3% (3/1056).
The topological predilection of the appearance of DL roots in the mandibular molars has been discussed in many studies. However, this issue still remains controversial. Bilateral DL roots have been reported in 37.14%-67% of cases.57 However, some researchers have reported a higher prevalence of DL roots on the right side,131519 whereas other researchers have found DL roots to be more prevalent on the left side.2021 Most previous studies involving Korean subjects showed that DL roots were more prevalent on the right side,1516 and the present study confirmed those results. The conflicting results of the studies conducted in different populations may be due to differences in sample size, case selection, or methodology,3 and more studies are necessary to assess this issue.
DL roots in the mandibular molars have been reported to be short and highly curved in comparison with other roots, but insufficient information about the length of DL roots has been reported. According to a study carried out by Chen et al.22 that used 293 extracted human mandibular first molars, the mean length from the distal furcation to the root apex in DL roots was 6.3±1.6 mm, whereas the corresponding length in DB roots was 7.8±1.8 mm. This discrepancy was statistically significant. Gu et al.11 analyzed the vertical length of DL roots using micro-CT and reported that DL roots were shorter than DB roots and mesial roots. The present study used CBCT images to measure the vertical length from the canal orifice to the root apex of the DL root, and our results correspond to those of previous studies.
The interorifice distance between the DB canal and the DL canal affects the design of the access cavity. If a DL root is present, the shape of the access cavity must be changed from its typical triangular shape to a trapezoidal shape.713 Compared to the typical DL canal in two-rooted molars, the orifice of the DL canal of a three-rooted molar with a DL root is located more distolingually. Gu et al.8 measured the mean interorifice distance between the DB and DL canals of three-rooted molars. They found that the mean interorifice distance was 2.9 mm, which was similar to the results of the present study (2.8±0.2 mm). Theoretically, the DL corner of the access cavity must form an angle of 75°,8 but in cases where a DL root is present, the expansion of the cavity in the lingual direction makes it easy to locate the canal orifice.4
Previous studies that performed a quantitative analysis of DL root curvature found that DL root curvature was different in the BL orientation than in the MD orientation.622 Chen et al.22 reported the results of measuring the DL root curvature of the mandibular first molar by Schneider's method, using a radiograph in the BL and MD directions. According to their results, most DL roots had a larger angle of curvature in the BL orientation (36.4°±9.4°) than in the MD orientation (9.2°±6.1°). They also found that most of the DL roots showed severe curvature, and 28.6% of them had curvature in the apical third. In addition, according to the canal curvature measurements performed by Gu et al.6 in the clinical view and in the proximal view, the DL canal curvature was larger in the proximal view (36.4°) than in the clinical view (9.2°). However, it was found that both the BL curvature and the MD curvature could appear larger in the apical two thirds of the DL root.513 In the present study, the DL root curvature appeared larger in the MD orientation in the coronal portion of the root; but in the apical portion, it appeared larger in the BL orientation.
An anatomical variation of this type implies that instrument separation may occur easily at the time of instrumentation. In addition, since conventional radiographs may not enable the acquisition of information about curvature in the BL orientation, the angled radiographic technique is considered necessary for accurate diagnosis. Wang et al.23 suggested that an additional 25° mesial horizontal angulated radiograph is necessary to accurately diagnose DL roots.
As demonstrated in many studies, coronal flaring decreases the curvature angle of the coronal root around the root canal orifice. For access to the apical third at the time of endodontic treatment, it is recommended to decrease the curvature angle through sufficient coronal flaring.6 However, since most DL roots are short and curved and can therefore be weakened by excessive flaring and by the removal of remaining dentin, care must be taken to prevent the occurrence of vertical root fracture.7
The present study investigated the concurrent appearance of a DL root in the mandibular first molar and a Cshaped canal in the mandibular second molar, which are anatomical variations that are both known to be prevalent among East Asians. No correlation was identified between the presence of a DL root in the mandibular first molar and the presence of a C-shaped canal in the mandibular second molar. However, the appearance of a C-shaped canal in the mandibular second molar showed a general tendency to be bilateral, regardless of the presence of a DL root in the mandibular first molar.
In this study, a high prevalence of DL roots in the mandibular molars was found, and the observed DL roots were mostly in the mandibular first molar, with a tendency to be bilateral. Moreover, no correlation was found between the presence of a DL root in the mandibular first molar and the presence of a C-shaped canal in the mandibular second molar. In cases where a DL root was observed in the mandibular molars, the root canal curvature in the MD orientation was significantly different than in the BL orientation. Therefore, when treating mandibular first molars, especially in East Asian patients, clinicians should be aware of the possible existence of a separate DL root and assess the characteristics of the curvature of the root canal prior to treatment.
Go to :
 XML Download
XML Download