

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With edentulous patients, it is difficult to secure suitable positioning when taking panoramic radiographs and also it is hard to assess the positioning by means of inspecting anatomical structures such as the occlusal plane, antero-posterior position of the anterior teeth, and symmetry in their panoramic radiographs after taken. Several studies have examined the difficulties of taking panoramic radiographs of edentulous patients. Without distinguishing between dentulous and edentulous images, Dhillon et al.1 noted that most panoramic radiographs had at least one error. Glass et al.2 reported that 89% of panoramic radiographs of edentulous patients had at least one error, which included the following positions: chin too high, too far forward, tongue not raised, chin too low, head tilted, head turned, and too far back. Batenburg et al.3 showed that panoramic radiographs without positioning reproducibility were not reliable for diagnosis and evaluation of the edentulous mandible. Accuracy and reproducibility of edentulous patients' panoramic radiographs are important for dental diagnosis and treatment planning because panoramic radiographs have been widely used in cases of the screening of cysts, foreign bodies, and neoplasms,456 finding bone resorption and osteopenia of the jaws,789 and installing implants.10
Conventional bite blocks and chin-support devices, such as the ones included with the Orthopantomograph® OP100 (Imaging Instrumentarium, Tuusula, Finland) (Figs. 1A and B, respectively), are widely available for positioning anterior edentulous patients during panoramic radiography.11 The chin-support device is more commonly used than the conventional bite block because the height of the bite block is 12 mm, which seems to provide an insufficient vertical dimension for the edentulous area.
However, using the chin-support device for panoramic radiography has also presented some problems. Panoramic radiographs using the chin-support device have frequently shown insufficient inter-maxillary space and lack of reproducibility (Fig. 2). According to the study of Park et al.,12 the reproducibility of panoramic radiographs of edentulous patients using a conventional chin-support device was worse than that of dentulous patients. Therefore, a new bite block for edentulous patients is required to improve the accuracy and reproducibility of panoramic radiographs of edentulous patients by improving the accuracy and reproducibility of positioning patients for taking panoramic radiographs.
The aim of this report is to propose a new bite block for panoramic radiographs of edentulous patients that could enable a greater degree of accuracy and reproducibility in patient positioning, and reduce the weaknesses of panoramic radiographs taken with a chin-support device.
Materials and Methods
A new bite block for edentulous patients was designed to bring reproducibility when taking panoramic radiographs to a similar level as that of a bite block for dentulous patients. The new bite block for edentulous patients involved modifications in the bite portion that could compensate for the missing anterior teeth and resorbed anterior alveolar bone tissue of anterior edentulous patients. The dimensions of the missing and resorbed tissues were determined by referring to previous studies.
In detail, the new bite block (Fig. 3A) was designed to position anterior edentulous patients in the same manner as anterior dentulous patients who could bite into the notches of a conventional standard bite block (Fig. 3B) while undergoing panoramic radiography. The new bite block needed to compensate for the area of missing anterior teeth and resorbed alveolar bone. To compensate for those areas, statistical analysis of measured tooth lengths, facio-lingual inclinations, and resorbed anterior alveolar bone dimensions were investigated in the literature. According to Volchansky and Cleaton-Jones,13 the mean sizes of teeth were 10.0 mm among the maxillary central incisors and 8.4 mm among the mandibular central incisors in those aged 20 to 40 years. Furthermore, the mean facio-lingual inclination of the maxillary central incisors was 33.50°, and that of the mandibular central incisors was 26.44°.14 The mean angle between the occlusal plane and Frankfort horizontal plane was 6.79°.15 Thus, the angle between the maxillary central incisor and vertical plane was 26.71°, and the angle between the mandibular central incisor and vertical plane was 19.65°. Also, the extent of anterior alveolar bone resorption was 5.90 mm in non-denture wearers and 6.69 mm in denture wearers in the maxillary central incisor area, and 7.07 mm in non-denture wearers and 13.03 mm in denture wearers in the mandibular central incisor area.16
Using these values, the vertical dimension and the antero-posterior horizontal distance (horizontal distance) of the new bite block was determined. For the vertical dimension, the vertical vector of the anterior tooth portion was calculated to be 16.85 mm, and the thickness of the bite position (notch) of the conventional standard bite block for dentulous patients of the Orthopantomograph® OP100 (2 mm) was taken into consideration. Thus, the vertical height of the new bite block was chosen to be 18.85 mm, and adjusted to 18 mm by trial and error (Fig. 4). For the horizontal distance, which is the difference between the lengths from the panoramic radiograph sensor to the standard block's notch and to the biting position of the new bite block, the horizontal vector of the anterior tooth portion was calculated to be 4.49 mm, and the horizontal vector of the resorbed bone portion was considered to be in the range from 2.65 mm to 3.00 mm. The horizontal distance for the new bite block was chosen to be 5 mm (4.49 mm), and was adjusted to 7 mm by trial and error (Fig. 4).
Panoramic radiographs of anterior edentulous patients were taken using the new bite block. Then, the panoramic radiographs were compared with the radiographs taken previously using conventional chin-support device. Then the reproducibility and technical errors of the radiographs using the conventional chin-support device were evaluated and compared to the radiographs using the new bite block.
Results
Some radiographs taken with the chin-support device have shown insufficient inter-maxillary space (Fig. 5A), and others have lacked reproducibility of anatomical structural dimensions, especially in the horizontal direction (Fig. 5B). The chin-support device might not provide appropriate reproducible and accurate positioning in taking panoramic radiographs.
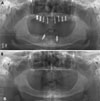
Panoramic radiographs taken with the new bite block showed better stability in inter-maxillary vertical space, antero-posterior position, and bilateral symmetry than radiographs taken with the conventional chin-support device (Fig. 6). In addition, according to the radiographers' statements, the patients using the new bite block showed less movement and more stable positioning while undergoing panoramic radiography.
Discussion
The panoramic radiographs of edentulous patients taken with the chin-support device showed some errors. These problems could have originated from the unreliability of the chin-support device in positioning patients while undergoing panoramic radiography. In other words, the chin-support device would provide inappropriate reproducibility and inaccurate positioning support. This finding was in accordance with those of Park et al.,12 justifying the attempt to design a new bite block for panoramic radiographs of edentulous patients. Therefore, this new bite block was designed and implemented, and a patent was obtained on the bite block in the Republic of Korea (Registration No. 1299456).
The new bite block produced better inter-maxillary space, antero-posterior position, and bilateral symmetry in panoramic radiographs than the conventional chin-support device. These results might have originated from stable and accurate positioning of both of the jaws in taking panoramic radiographs with the new bite block.
However, ongoing evaluation of the new bite block should be carried out, including assessment of image quality and reproducibility. It will take time to accumulate panoramic radiographs taken with the new bite block in order to perform these assessments.





 XML Download
XML Download