

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Vertical root fracture (VRF) is characterized by a fracture line originating from the apex of the tooth and extending toward the coronal section. Root canal therapy has been shown to be one of the primary etiologies of VRF, and hence, the incidence of VRF in endodontically treated teeth varies between 3.7% and 30.8%.1,2,3 Since VRF significantly worsens the prognosis of the tooth, it is crucial to detect fractures prior to performing further treatments such as restorations, root canal retreatment, or apicoectomy.
Based on the results of previous studies, we know that computed tomography (CT) and cone beam computed tomography (CBCT) have higher diagnostic values for the detection of VRF than conventional radiography. Furthermore, CBCT has been shown to have comparable diagnostic values to CT at a lower cost and lower absorbed radiation for the patient. As a result, its application is becoming significantly more common.4,5,6,7,8
Nonetheless, due to the image capturing and reconstruction techniques of CBCT, metallic structures can cause artifacts in the images.9 Since most teeth suspected to have VRF are endodontically treated and have a metallic post in the root canal, VRF detection may pose a challenge. Most intracanal posts are manufactured using stainless steel or titanium; therefore, this study compared the sensitivity, specificity, and diagnostic accuracy of VRF detection in teeth without posts and in those with stainless steel or titanium posts, by using a CBCT system.
Materials and Methods
Extracted single-rooted, closed-apex human teeth were used in this study. The reasons for tooth extraction, age, and gender of the patients had no effect on the study and were therefore not considered to be variables in this study. The absence of an existing fracture was confirmed by methylene blue staining (Aldon Corporation, Avon, NY, USA). The teeth were randomly divided into two groups: root fracture was induced in the first group, while the second group was kept intact. In order to induce the fracture, the roots were covered with 1 mm of wax (Dental Wax, Maves Co., Cleveland, OH, USA) and were embedded in acrylic blocks (Technovit 4000, Heraeus Kulzer, Wehrheim, Germany). Pre-fabricated titanium posts (AZtec Anchor, Dentatus, New York, USA) of equal length (10.5 mm) were inserted into the root canals. Force was applied on the posts by using the Instron Testing Machine (Zwick/Roell 7020; Zwick, GmbH & Co. KG, Stuttgart, Germany) until the root fracture occurred (Fig. 1). The amount of force required for the root fracture was recorded in newtons (range: 200-300 N). The moment of fracture was determined by a sudden drop in force on the post in the Instron machine diagram (Fig. 2). In order to confirm the fracture, the teeth were extracted from the acrylic block and stained with 1% methylene blue (Aldon Corporation, Avon, New York, USA). If the fractured segments became separated from the root in a sample, the tooth was excluded from the study. In total, 80 teeth were included in the study, of which 40 teeth contained a fracture and 40 had no fracture.
The teeth were then randomly mounted on four acrylic casts (20 in each cast), simulating the human mandible (Fig. 3). The acrylic casts (Technovit 4000, Heraeus Kulzer, Wehrheim, Germany) were fixed in a horseshoe shape at a height of 3 cm and width of 2 cm, and with 0.5 cm of acrylic around each root. All four casts were scanned with the NewTom CBCT system (NewTom VG, Quantitative Radiology, Verona, Italy) three times (field of view (FOV): 8 cm×12 cm, 110 kVp, 13.8 mA, 18 s, voxel size: 0.15 mm). The first scan was completed without posts (NP condition), the second was completed with titanium posts (AZtec Anchor 10.5 mm, Dentatus, New York, USA; TP condition), and the third with stainless steel posts (Classic Surtex 10.5 mm, Dentatus, New York, USA; SSP condition) (Fig. 4).
The images were analyzed by two oral and maxillofacial radiologists with more than five years of experience and by two endodontists with more than seven years of teaching experience, who each viewed the images twice. All participants viewing images were blinded to the study groups. The interval between the two analyses by each viewer was four weeks. The internal software of the CBCT machine was used to view the images (NNT Viewer, Quantitative Radiology, Verona, Italy). All images were displayed on a 21.3-inch true-color flat-panel monitor (SyncMaster 213T, Samsung, Seoul, Korea) at its native resolution of 1600×1200 pixels under dimmed ambient lighting. All observers had a calibration session prior to their assessments where they were given the opportunity to adjust the contrast and the brightness of the images and were able to view multiple cross sections of each image with no time limit. The sensitivity, specificity, and accuracy of the diagnosis were evaluated in each group for each observer by ANOVA, Tukey's HSD, and a kappa test using SPSS version 16.0 (IBM Co., Armonk, New York, USA).
Results
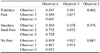
When comparing the results of the radiologist readings, the sensitivity, specificity, and accuracy differed significantly among the NP, TP, and SSP conditions (p=0.041, 0.02, 0.039, respectively). The accuracy and the specificity of detection were significantly higher under the NP condition than under the SSP condition (p=0.023 and 0.001, respectively). The sensitivity of VRF detection was significantly higher under the NP condition than under the TP and SSP conditions (p=0.048 and 0.016, respectively) (Table 1).
The results of the endodontist group showed a significant difference in the accuracy and the sensitivity between the conditions (p=0.036 and 0.04, respectively). The accuracy was significantly higher under the NP condition than under the SSP condition (p=0.021), while the sensitivity was significantly lower under the SSP condition than under both the NP and the TP conditions (p=0.034 and 0.042, respectively) (Table 2).
When the analyses by radiologists and endodontists are combined, the sensitivity, specificity, and accuracy showed a statistically significant difference among the three conditions (p=0.03, 0.07, and 0.04, respectively). Accuracy and specificity were significantly higher under the NP condition than under the SSP and the TP conditions (p=0.001 and 0.014 for accuracy and 0.036 and 0.001 for specificity, respectively). Sensitivity was significantly higher in the case of NP than in the case of SSP (p=0.04) (Table 3).
A comparison of the results of the radiologists with those of the endodontists showed a statistically significant difference in terms of sensitivity. The mean sensitivity reported by the radiologists was significantly lower for the TP and the SSP conditions and significantly higher for the NP condition (p=0.012, 0.014, and 0.022, respectively). Accuracy and specificity followed the same pattern; however, the differences were not statistically significant.
Intraobserver agreement was calculated between the first and the second analyses of each observer using the kappa agreement coefficient (Table 4). The highest level of agreement was observed for the NP condition. Interobserver agreements between different groups were measured using the kappa agreement coefficient (Table 5). The highest average agreement was measured under the NP condition followed by the SSP and the TP conditions.
Discussion
Despite the numerous advantages of CBCT for the diagnosis of a root fracture, the clinical application of this technique is associated with some limitations,10 particularly in teeth with intracanal metal posts. In some cases, metallic artifacts associated with intracanal posts may be misdiagnosed as root perforations or fractures.11 In this study, the condition without an intracanal post showed a higher sensitivity, specificity, and accuracy than the conditions with intracanal posts.
In this study, materials with lower X-ray beam attenuation coefficients (density), such as titanium, caused fewer metallic artifacts than materials with higher densities such as stainless steel.12 The present study also demonstrated that the use of titanium posts was associated with fewer diagnostic errors in the detection of root fractures. This was in agreement with the results of Ferreira et al,13 which showed that fiber-resin posts have less of an effect on the diagnosis of a root fracture than titanium posts. Nonetheless, the sensitivity of VRF detection was not statistically different between the NP and the TP conditions; therefore, CBCT could be regarded as an appropriate technique for the diagnosis of root fractures, even in cases with titanium posts.
The relatively low specificity as compared to the sensitivity for the three conditions is associated with a risk of tooth loss following a misdiagnosis. As a result of low specificity, an intact tooth may be misdiagnosed for a fractured one and mistakenly extracted. Specificity was numerically higher under the TP condition than under the SSP condition, which suggests an advantage of the use of titanium posts in order to reduce errors in the detection of root fractures.
In contrast to this study, Youssefzadeh et al14 reported a higher specificity than sensitivity. The difference between the two studies may be attributed to the difference in sample size, number of observers, and study designs. Their study was an in vivo design with natural root fractures versus the in vitro design of this study with induced root fractures.14 When fractures are intentionally induced, the odds of the separation of the fractured margins are greater and the fracture pattern is more discernible than those in the case of natural fractures.
According to a study by Hassan et al,15 the presence of a root canal filling material had no effect on the sensitivity but reduced the specificity of detecting VRF. However, this study showed a decrease in both sensitivity and specificity under the TP and the SSP conditions as compared to the values under the NP condition. In another study by da Silveira et al,16 the presence of a root canal filling material or posts inside the canals had a more profound effect on the specificity than on the sensitivity. The intracanal posts demonstrated the same effect in the present study. Low specificity might originate from the artifact caused by the opaque materials that created a pattern simulating a fracture line, and result in a false positive diagnosis of VRF.
In contrast to this study, Taramsari et al showed that the frequency of VRF diagnosis was similar between teeth with fiber posts and screw posts.17 Moreover, they showed that the presence of intracanal posts decreased the diagnostic values of root fracture; however, the difference was only numerical without a statistical significance. In another study, Jakobson et al18 also reported that in most cases, metallic posts did not influence the sensitivity of the VRF diagnosis. Furthermore, they showed that CBCT had a higher sensitivity for root fracture diagnosis in roots with posts and buccolingual fractures. In a recent study, Moudi et al19 showed that the presence of gutta-percha in the canal does not decrease the accuracy of the VRF diagnosis and the addition of prefabricated posts in the coronal part of the canal only decreases the accuracy numerically and not significantly.19
In the present study, the observers were radiologists and endodontists. The diagnostic ability of the radiologists before the placement of posts was greater than that of endodontists. The situation was reversed after the placement of posts. This finding might be explained by the familiarity of endodontists with the radiographs of endodontically treated teeth. In other words, some cases of VRF remained undetected in the radiologists' observations. Nonetheless, the difference between the two groups of observers in terms of specificity and accuracy was not statistically significant.
When VRF is diagnosed, the treatment plan usually involves tooth extraction. Thus, it seems that a higher specificity in detecting fractures will lead to less harm to the patient than a higher sensitivity. Based on the results of this study, it is recommended that the diagnosis of root fracture be made by a multidisciplinary approach. In cases where endodontic consultation is not possible, a radiologist's opinion should be obtained. For all of the conditions under study, the obtained intraobserver agreements were above 50% and the highest level of agreement was in the teeth without posts followed by teeth with SSP and TP.
In conclusion, intracanal posts decreased the sensitivity, specificity, and accuracy of VRF detection. Stainless steel posts decreased the diagnostic values of VRF detection more than did the titanium posts. Moreover, the use of posts resulted in a reduction in the interobserver agreement for the detection of VRF.







 XML Download
XML Download