

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The mandibular canal is an important landmark that should be considered before any surgery in the posterior mandible.1,2,3 Preoperative radiological diagnosis can provide the exact location of the mandibular canal and thus prevent complications during any surgical procedures.4 The course of the mandibular canal has been investigated in several studies, and frequent anatomic variations have been found in the intrabony course of the inferior alveolar nerve.5,6,7 Further, the radiographic appearance of the mandibular canal can be variable.8
The visibility of the mandibular canal may vary significantly, even within the same individual.9,10,11 Wadu et al11 found that in a reasonable number of cases, the radiopaque border is disrupted in radiographic images, and it is invisible in some other cases. The mandibular canal is usually formed by a thin trabecular bone with many circumferentially located voids, and there is a thin layer of cortical bone in only a few mandibles.12,13 Radiological analyses have suggested a correlation between alveolar bone quality and the presence of the mandibular canal wall.14
Previous studies have investigated the visibility of the mandibular canal using panoramic radiography, computed tomography, or cone-beam computed tomography (CBCT).1,15,16,17,18,19,20 On panoramic images, the mandibular canal is typically seen as a well-defined radiolucent zone, lined by radiopaque superior and inferior borders.4 Several researchers have found it difficult at times to identify the mandibular canal on panoramic images.15,16,17,18,19 Computed tomography4,15,16,17 and CBCT1,20 have been superior to conventional imaging modalities for the depiction of the mandibular canal. As a general rule, if the inferior alveolar is poorly depicted on panoramic radiographs, the canal will be difficult to localize using other imaging modalities.21
The understanding of the anatomic variability of the course and visibility of the mandibular canal will be helpful in treatment planning for procedures involving the posterior mandible.22 The aim of this study was to investigate the course of the mandibular canal on panoramic radiographs and to assess the visibility of this canal on panoramic radiographs and CBCT cross-sectional images.
Materials and Methods
In this retrospective study, the samples were chosen randomly from patients who visited Pusan National University Dental Hospital and underwent panoramic radiography as well as CBCT in 2013. The CBCT scans had been taken as part of a clinical diagnostic procedure for various reasons, such as implant placement, extraction of the third molar, or orthodontic treatment planning. The patients were 140 males and 122 females with a mean age of 29.4 years (age range: 20-60 years). Subjects with mandibular pathology were excluded from the study.
All panoramic radiographs were taken using a Proline XC (Planmeca Co., Helsinki, Finland). CBCT scans were acquired using a PaX-Zenith 3D (Vatech Co., Hwasung, Korea). The scanning parameters were 100-105 kVp, 24 s, 5.0-5.6 mA, voxel size of 0.2 mm, and field of view of 16 cm×14 cm. CBCT images were processed and observed with Ez3D Plus Professional K software (Vatech Co., Hwasung, Korea). Cross-sections were perpendicular to the dental arch, and the occlusal plane served as the reference for cross-sections. The observer carefully examined these images, scrolling through consecutive cross-sectional images.
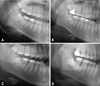
The course of the mandibular canal, as seen in the panoramic radiographs, was classified into four types: linear, elliptic, spoon-shaped, and turning curves (Fig. 1).23 The visibility of the mandibular canal was evaluated by visually determining whether the mandibular canal was clearly visible, probably visible, or invisible on panoramic radiographs and CBCT cross-sectional images (Fig. 2). It was assessed in three mandibular regions: the first molar, second molar, and third molar regions. The visibility of this canal on panoramic radiographs was compared with that on CBCT images.
Descriptive statistical analysis was applied to the data. The Wilcoxon signed-rank test was used to detect statistically significant differences in the visibility of the mandibular canal between the right and the left sides, and between panoramic radiography and CBCT. The Kruskal-Wallis test was used to examine the difference in the visibility of this canal according to the course of the canal and the difference in visibility in the three mandibular regions. A p value of less than 0.05 was considered to indicate a statistically significant difference. Statistical analyses were performed using IBM SPSS Statistics 21.0 (IBM, Armonk, NY, USA).
Results
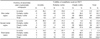
There was no statistically significant difference between the right and the left sides, and the results of both sides were averaged. Elliptic curves were most frequently observed along the course of the mandibular canal (p<0.05) (Table 1). The percentage of clearly visible mandibular canals was highest in spoon-shaped curves and the lowest in linear curves (Tables 2 and 3).
On panoramic radiographs, the percentage of invisible mandibular canals was 22.7% in the first molar region, 11.8% in the second molar region, and 1.3% in the third molar region. On CBCT cross-sectional images, the percentage of invisible mandibular canals was 8.2% in the first molar region, 5.7% in the second molar region, and 0.2% in the third molar region. In the first molar region, the percentage of clearly visible mandibular canals was 13.0% and 50.4% on panoramic radiographs and CBCT, respectively. The CBCT cross-sectional images were significantly better than the panoramic radiographs in assessing the visibility of the mandibular canal (p<0.05). The visibility of this canal in distal regions was significantly better than in the first molar region (p<0.05) (Table 4).
Discussion
In this study, the course of the mandibular canal was investigated on panoramic radiographs, and the visibility of the canal was assessed on both panoramic images and cross-sectional CBCT images. Our results showed the variation in the course and visualization of this canal.
Several researchers have classified the course of the mandibular canal according to the vertical locations within the mandible, such as high, low, and intermediate locations. 6,7,24 In a study using 96 plain films of dried mandibles, Heasman showed that a majority (68%) of inferior canals passed along an intermediate course between the root apices and the inferior border of the mandible.24 Ozturk et al22 confined classification to the canal's course in the mandibular body: straight projection (12.2%), catenary-like configuration (51.1%), and progressive descent from posterior to anterior (36.7%). This study classified the course of the mandibular canal into linear, spoon-shaped, elliptic, and turning curve types, as in the study conducted by Liu et al.23 A linear curve (22.9%) in our study was very similar to the straight projection (12.2%) observed by Ozturk et al, and the other curves were not similar to their findings.22 In the study conducted by Liu et al,23 elliptic curves (48.5%) were the most common, and spoon-shaped curves (29.3%) were the next most common course. The most common course found in our study was an elliptic curve (64.7%), and this was followed by linear (22.9%) and spoon-shaped curves (6.9%). Elliptic and spoon-shaped curves could provide more space for implant placement than linear curves.
The visibility of the mandibular canal may vary between patients and between different areas of the mandible.1 Klinge et al15 reported that the mandibular canal of specimen cadavers was not visible in 36.1% of panoramic radiographs. Naitoh et al25 reported that on panoramic images, the canal was entirely invisible in 32% of the examined sites in the molar region. In our study, the mandibular canal was not invisible in 22.7% of the examined sites in the first molar region on panoramic radiographs. In addition, Lindh et al26 reported that the mandibular canal of specimen cadavers was clearly visible in 25% of panoramic radiographs. In this study, on panoramic radiographs, the mandibular canal was clearly visible in 13.0% of the examined sites in the first molar region and 46.8% of the examined sites in the third molar region. The depiction of the mandibular canal wall on panoramic images was related to the bone density in the alveolar region.25 Reduced visibility of the mandibular canal wall on a panoramic radiograph might indicate lower integrity of the mandibular canal wall and reduced bone trabeculation.27
The mandibular canal presented overall satisfactory visibility on CBCT cross-sectional images in most cases.1 De Oliveira-Santos et al14 reported that on CBCT cross-sectional images of the first molar region, corticalization of the mandibular canal was observed in 59% of hemimandibles, and in 23% of the cases, the canal was not corticalized but could be visualized. Our results showed that the mandibular canal was clearly visible in 50.4% of the examined sites in the first molar region on CBCT images and was probably visible in 41.4% of the sites. Further, the visibility of the mandibular canal differed according to the course of the mandibular canal on panoramic radiographs. The percentage of clearly visible mandibular canals was the highest in spoon-shaped curves and the lowest in linear curves.
CBCT was found to be superior to panoramic images for the identification of the mandibular canal.19 Kamrun et al4 confirmed that the visibility of cross-sectional CT images was significantly higher than that of panoramic images of the mandibular canal. Our results showed that the visualization of the mandibular canal on panoramic images was remarkably improved by the use of cross-sectional CBCT images.
The mandibular canal was more readily identified in posterior areas, and the visibility gradually decreased towards the mental foramen.1 The most frequently missing portion of the canal was the superior border apical to the first molar.10 The visualization of the canal in the posterior third of the mandibular canal was significantly better than that in the other areas on both panoramic and CBCT images.19 Our results showed that the visibility of the mandibular canal in the third molar region was better than that in the first molar region.
In conclusion, the visibility of the mandibular canal was affected by the course of the canal, and the percentage of clearly visible mandibular canals was the lowest in linear curves. Further, the visibility of the mandibular canal increased in more distal regions of the canal, and the canal was more visible on CBCT cross-sectional images than on panoramic radiographs.




 XML Download
XML Download