

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The popularity of cone-beam computed tomography (CBCT) has increased in recent years, with an increasing use for diagnosis and treatment planning in different fields of dentistry.1 The incorporation of cone-beam technology into clinical practice took place thanks to two main facts, namely the conversion to digital imaging and the progress in image acquisition, allowing detailed three-dimensional (3D) images. Images are now held on an axial matrix and can be displayed in axial, sagittal, or coronal views. They can also be seen in the traditional panoramic view or as 3D reconstructions.2
CBCT has different applications in dentistry and oral and maxillofacial surgery with some advantages: it allows the modification of the visual field, provides a high resolution thanks to a voxel size range of 0.076-0.4 mm, reduces artifacts caused by metals in conventional computed tomography, and generates a very low amount of radiation (particularly when compared with conventional computed tomography for medical use). The equipment design is becoming more ergonomic and easier to use, image distortion is minimal, and the images are compatible with other planning and simulation software due to their DICOM format.3,4
CBCT has recently begun to be used in dental root canal morphology analysis.5 Some applications in this field are as follows: anatomical variability of roots and root canals, diagnosis of dental traumatic injuries, periapical pathology, differential diagnosis with other pathologies, nonsurgical treatment of root canals, and presurgical treatment planning.6,7
Root canal anatomy of mandibular premolars and morphological differences between the first and the second premolars have been evaluated by using different procedures.8,9,10,11,12,13,14 Several studies have reported a large variation in the number of roots, root canal type, and apical foramina in mandibular premolars.8,11,12,13,14,15,16,17,18,19 Only a few studies, limited to the western Chinese and Korean populations, have evaluated the root anatomy of mandibular premolars using CBCT.14,20 According to Micheti et al.21 CBCT is a very interesting, reliable, noninvasive measuring technique that can be used in all spatial planes to study dental anatomy.
This study aimed to investigate the external and internal morphology of human mandibular premolar roots in a Spanish population by using CBCT and to correlate the findings with the patient's gender and the tooth type.
Materials and Methods
Sample selection
This study was approved by the Ethics Committee of the Faculty of Medicine and Dentistry of the University of Valencia (Valencia, Spain), and informed consent was obtained from patients whose scans were used.
This study consisted of 200 CBCTs taken from October 2011 to February 2012 for different diagnostic reasons, such as bone absence for implant placement, assessment of tooth root relationships with clinically relevant anatomical structures, dental surgery, and diagnosis of mandibular radiolucent lesions. The inclusion criteria were as follows: full view of one or more mandibular premolars, complete root formation, no resorption signs, no endodontic treatment performed, and no posts or coronal restorations. Finally, 70 CBCTs with 126 premolars were included in the study.
Image acquisition and assessment
For image acquisition, a Kodak 9000 3D unit (Carestream Dental, Atlanta, GA, USA) was used. Radiographic images were obtained by a radiodiagnostic technician according to the manufacturer's specifications (70 kV, 10 mA, and 10.8 s), which guaranteed the quality of the images with the lowest irradiation for patients.
Measurements were performed with CS 3D Imaging Software 3.1. (Carestream Dental, Atlanta, GA, USA), in the oblique cut, as it is the most appropriate for canal visualization, thereby obtaining a clear view of the three planes. Sections were performed at 76 µm(voxel size: 76 µm×76 µm×76 µm), with a screen resolution of 1366×768 pixels. One dentist and one radiologist evaluated the samples separately, and in cases where differences were found after discussion, another dentist was asked to perform a third evaluation and further discussion was conducted to reach a final consensus.
In order to select the images using which the measurements would be made, two reference planes, namely mesiodistal and buccolingual, were chosen. Therefore, mesiodistal root curvatures were assessed in the first evaluation and buccolingual curvatures were evaluated in the second evaluation. The axial plane was sliding from the chamber to the apical foramen, facilitating the observation of the possible canal divisions and forms. The contrast was adjusted when needed, and a zoom of between 0.4 and 1.1 was used.
Measurements
The evaluated variables were as follows: patient's age and gender, tooth position in the arch, number of roots, length of the tooth and root, number of canals, canal system configuration according to the Vertucci criteria22 distance from the cemento-enamel junction to the canal bifurcation and canal reunification (when it was the case), number of foramina, root curvature, angle location, and distance of the angle vertex to the apex.
The tooth length in the mesiodistal plane (maximum crown-apex distance) as well as the root length (from the mesial cemento-enamel junction to the apex) was measured with the linear measurement tool (Fig. 1A). A number of canals were observed by moving the coronal plane, checking them in the axial plane (Fig. 1B), and covering the tooth from the pulp chamber to the apex in order to confirm the observed configuration. With respect to the angles, each tooth was observed in the mesiodistal and buccolingual planes to check them and their orientation. Root curvature was measured in degrees, and the complementary angle was calculated to be 180°; the distance from the angle vertex to the apex in millimeters was also measured (Fig. 1C).
Statistical analysis
Data were tabulated and analyzed using IBM SPSS statistical package 19.0 (IBM Co., Chicago, IL, USA). A descriptive analysis of the data was performed. Qualitative variables were compared using a chi-squared test, and an analysis of variance (ANOVA) test was used for comparing the qualitative and the quantitative variables. The significance level was p<0.05 in all the cases.
Results
The final sample size was 70 patients who underwent CBCT - 31 (43.7%) women and 39 (56.3%) men - with an average age of 45.26 years (confidence interval (CI): 32.12-58.71). The number of mandibular premolars was 126. The number of root canals is given in Table 1. All the elements in the sample were single-rooted teeth. The mean length of the teeth was 22.18 mm ranging from 21.87 to 22.49 mm (men: 22.79 mm, CI: 22.39-23.18; women: 21.39 mm, CI: 20.98-21.89). The teeth of the men were significantly longer than those of the women (p=0.00). The mean length of the first premolars was 22.3mm(CI: 21.83-22.97) and that of the second premolars was 21.8mm(CI: 21.23-22.51).
The mean length of the roots was 15.56mm(CI: 15.25-15.86) (men: 16.05 mm, CI: 15.64-16.46; women: 14.91 mm, CI: 14.50-15.32). The roots of the males were significantly longer than those of the women (p=0.00). The mean length of the roots was 15.60mm(CI: 15.18-16.14) for the first premolars and 15 mm (CI: 14.62-16.11) for the second premolars, without any statistically significant differences between them (p>0.05).
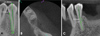
There were 105 teeth (83.3%) with one canal, 20 (15.9%) with two canals (Fig. 2A), and just 1 (0.8%) with three canals (Fig. 2B). In this case, the differences between men and women were not significant (p=0.34). There were no statistically significant differences between the first and the second premolars (p=0.21), but the first premolars showed more than one canal in more cases than the second premolars (Table 1).
Canal configurations according to the Vertucci criteria are listed in Table 2. Most of the teeth were type I, and the following most prevalent situation was type V distribution (Fig. 2C). One tooth showed a root canal configuration, not included in Vertucci's classification (one canal in the coronal third of the root, three canals in the middle third, and one canal in the apical third). Variability was significantly higher in the first premolars than in the second premolars (p=0.03). No difference by gender was detected (p=0.29). In cases where bifurcation was found, it was located at 6.87 mm (CI: 3.77-10.01) from the cemento-enamel junction. Canal confluence, when present, was found at 10.07mm(CI: 9.37-12.77) of the cemento-enamel junction. 89.7% of the teeth showed a single apical foramen (113 teeth), and the remaining 10.3%, two apical foramina (13 teeth, 9 of them in women, 69.2%). A significant association was found between the number of foramina and the female gender (p=0.04). 12.3% of the first premolars and 7.5% of the second premolars showed two foramina (p=0.55).
Data for root curvature are presented in Table 3. They were detected in 65% of the sample with no significant gender association (p=0.06), although 62.3% of the angulated teeth belonged to men. There were no significant differences between the first and the second angulated premolar percentages (p=0.32). Distal curvature was the most prevalent for the first premolars (30.1%), whereas buccal curvature was the most prevalent for the second premolars (22.6%), without any significant differences (p=0.67). With respect to the curvature position, there was no significant difference between men and women (p=0.21).
In the angulated teeth, an angle lower than 20° was found in 67 teeth (87.0%) and an angle greater than 20° in 10 cases (13.0%), without any significant differences for gender (p=0.23) or tooth. When the curvature was greater than 20°, the angle vertex was found at less than 5 mm from the apex (Table 4).
Discussion
The complex anatomy of the canal system in the mandibular premolars makes it difficult to assess their clinical morphology with conventional radiography.23 In most clinical situations, when using conventional radiological procedures such as periapical radiographs, the presence of morphological variations in the anatomy of the root canals can only be supposed when a change in shape or direction is detected, or when the root canal is not completely seen.24
With the use of the CBCT equipment, it is possible to obtain images with sufficient resolution to allow the study of the canal system anatomy, as performed in the present work. Although no specific tools for a root canal system study have been developed to date, the ones available for measurements in other dental applications have turned out to be suitable for this study. Micheti et al21 found an excellent correlation between CBCT reconstructions obtained with Kodak 9000 3D and the corresponding histological sections, claiming that CBCT is a reliable technique for the analysis of the root canal system anatomy.
Although there are few studies in this regard, some authors have used CBCT to study variations in dental anatomy in different series of teeth.25,26,27,28,29,30,31 In particular, the anatomy of the mandibular premolars has been studied using CBCT in the Chinese and Korean populations.14,20
The mean length of premolars as found in this study was 22.18 mm. The premolars of males were significantly longer than those of women, and the same trend was observed for the root length; this gender difference has not been analyzed in other studies reported thus far. The length of the second premolars was somewhat lower than that of the first premolars, but without any significant differences, these data are consistent with the findings of a study performed on the extracted teeth of a Jordanian population by Awawdeh et al.25 However, other studies32,33 found almost identical lengths for both teeth, possibly because these studies used radiographs and the present study used CBCT.
The most frequent morphology found in our study was one root and one canal, in accordance with the findings of other researchers.11,12 The results of studies in different ethnic populations with different procedures also agreed with these results; nevertheless, cases of other situations including C-shaped canals, more than one root, or more than two canals have described very rarely.12,14,34,35 Although no significant difference was found between the first and the second premolars with respect to the number of canals, the prevalence of two canals was higher in the first premolars than in the second premolars, 20.5% versus 4.5%, as described by Yu et al.20
The most prevalent root canal configuration observed in our study was Vertucci type I, followed by type V, with a higher morphological variability in the first premolars. 21% of the canals showed some kind of bifurcation, located at 3.77-10.01 mm from the cemento-enamel junction (middle/apical root thirds). These results are consistent with those found in the literature by other researchers.20,23,35
Root curvature was more prevalent in the first premolars than in the second premolars, with distal curvature being the most observed in the first premolars, a situation similar to that described by Khedmat et al in an Iranian population23 although the prevalence of deviation found in our population was higher, 30.1% versus 17.5%. Further, in our study, the curvature angle was lower than 20° in the first and the second premolars in 91.7% and 79.3% of the cases, respectively. In the few cases where the angle was larger than 20°, it was always found at less than 5 mm from the apex (Table 4). These results are in accordance with those obtained by Willershausen et al in 200936 wherein the angle ranged between 13° and 19° and the last curvature was done at less than 5 mm from the apex. This configuration is important as it is a factor increasing the difficulty of the root canal treatment in the teeth with the highest curvatures close to the tooth apex.37
In the present study, we found a higher prevalence of two foramina in women than in men, something not detected in the literature review. The higher prevalence of more than one foramen in the first premolars (12.3%) than in the second premolars (7.6%) found in our work, is in agreement with the results presented in an extensive series published in two literature reviews, but there, the percentages were higher for both tooth types.11,12
It can be concluded that CBCT was useful for evaluating the anatomy of mandibular premolars. Premolar lengths for men were greater than those for women. The first premolars showed a higher anatomical variability than the second premolars. The most prevalent Vertucci configuration was type I, followed by type V, with a higher variability in the first premolars than in the second premolars. Most teeth had a single foramen, and women had a higher prevalence of two foramina than men.





 XML Download
XML Download