

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Early diagnosis of primary dental caries and limitation of its harmful effects is the first concern in epidemiological studies.1,2,3,4 In daily clinical work, if we exclude sophisticated new methods, radiographic examination is the most frequently recommended method as a supplement to clinical inspection in the assessment of carious lesions.5,6 This recommendation is particularly emphasized in the assessment of proximal caries.7
Although digital radiography has replaced conventional (film-based) radiography to a varying extent in the developed and the developing countries due to its advantages,8,9,10,11 the degree of accuracy of both techniques in caries assessment is not consistent; one of them was considered superior in some studies,12,13,14,15 but other researchers believed that there was no significant difference between conventional and digital radiography with respect to caries assessment.16,17,18,19,20
Radiographic assessment of dental caries depends to a large extent on the visual and geometric characteristics of the image. One of these visual characteristics is image contrast.21 Tube voltage (kilovoltage peak; kVp) is the main factor affecting the image contrast; low kVp provides a short-grayscale and high-contrast image, while increasing kVp is indicated when a long-grayscale and low-contrast image is required.22,23
"A radiograph with a high contrast is useful for the detection and progression of dental caries."; "Some dentists prefer radiographs with a short-grayscale contrast, thinking that dental caries is easier to recognize.": These statements are part of oral radiology textbooks.24,25,26,27 It is important to determine whether this assumption is still valid and whether this validity is equal for digital images and conventional radiographs.
The aim of this study was to investigate the effect of changing tube voltage on caries assessment based on digital and conventional radiographs.
Materials and Methods
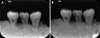
This study was conducted on 150 proximal surfaces of 75 human posterior teeth that were extracted for periodontal or orthodontic reasons. The selected teeth were visually sound or with proximal caries without occlusal cavitation and without extended buccal or lingual/palatal caries. Sets of three teeth each were mounted in contact in a mold made of plaster of Paris (Gipsina, Giza, Egypt). The level of gypsum was adjusted to be below the cemento-enamel junction of the examined teeth by 1-3 mm. A small piece of lead foil was attached to the tube side of the mold to indicate the mesial side of each image. All teeth were radiographed twice by using an intraoral X-ray machine (Minray, Soredex, Tuusula, Finland) set once at 60 kVp and the other time at 70 kVp. The tube current was 7 mA. The focus-to-film distance as well as the tube angulation between the central rays and the image receptors was fixed by using a simple cylindrical device. Eight 1.5-mm-thick layers of pink wax, leading to a total thickness of 12 mm, were placed between the position-indicating device (PID) and the teeth to simulate the effect of soft tissues in the oral cavity.28 Two types of image receptors were used to expose the investigated teeth in this study: E-speed films (CEA ID, Agfa Healthcare, Mortsel, Belgium) with a spatial resolution of 20 lp/mm, and a photostimulable phosphor plate (PSP) for a direct digital system (Digora Optime, Soredex, Tuusula, Finland) with a spatial resolution of 12.5 lp/mm and 14-bit grayscale (Fig. 1).
To choose the most appropriate exposure time, different exposure times were tested for each receptor. The shortest exposure times that produced high-quality images, as judged by three examiners, were included in the experiment. Conventional films were processed by an automatic processor (Extra-X, Velopex, London, England).
After being detached from their molds, the teeth were longitudinally separated (mesiodistally) at the middle of their proximal surfaces by using a water-cooled diamond saw. The separated crowns were examined under a stereomicroscope (Leica S 8APO, Microsystem, Heerbrugg, Switzerland) (Fig. 2).
All radiographic images were blindly assessed by three oral radiologists having more than five years of experience each, with a haphazard arrangement of the images. Each image was assessed twice with a period of two weeks between the two sessions. The radiographic images were evaluated inside a quiet room with dimmed light. A black cardboard with a customized window was placed on a viewer box to be used in the assessment of conventional radiographs, and the use of a magnifying lens (2× magnification) was allowed. The digital images were evaluated in such a room by using the Digora for Windows 2.7 software on an 18.5-inch monitor (SyncMaster B1930N, Samsung, Seoul, South Korea) with a resolution of 1360×768. The examiners were not allowed to change the contrast and the brightness of the images. Every interpretation session was terminated after 30 min or upon request of any of the examiners because of eye fatigue.
A five-point scoring system was used in the assessment of carious proximal surfaces as follows: 0: sound, 1: incipient caries (less than half the enamel thickness), 2: moderate (more than half the enamel thickness but does not reach the dentino-enamel junction), 3: advanced (less than half the dentin thickness), and 4: severe (more than half the dentin thickness).
The results of radiographic images were compared with those yielded by a stereomicroscope as the gold standard in order to calculate the sensitivity, specificity, positive predictive value (+PV), and negative predictive value (-PV) of both the investigated kVp values in the conventional and the digital images. The receiver operating characteristic (ROC) curve was used to evaluate the diagnostic accuracy measures of the different modalities. Areas under the ROC curve (AUCs) of the different tests were compared using a z-statistic. Inter- and intra-observer agreements (reliability) were assessed using the kappa statistic. The ROC curve analysis and the reliability analysis were performed with MedCalc Version 11.3 for Windows (MedCalc Software BVBA, Ostend, Belgium).
Results
Stereomicroscopic findings, the standard reference, revealed that 46.7% of the examined surfaces were carious, while the remaining 53.3% were sound. From the carious surfaces, 31.4% were confined to the enamel (14.3% incipient caries and 17.1% moderate caries) and 68.6% extended into the dentin (25.7% advanced caries and 42.9% severe caries).
With respect to the diagnostic accuracy measures and ROC curve analysis for caries detection using the two imaging modalities and the two kVp settings, conventional radiography (60 kVp) showed the highest sensitivity (74.3%), the highest -PV (77.8%), the highest diagnostic accuracy (77%), and the highest AUC (0.765). Conventional radiography (70 kVp) showed the highest specificity (86.3%) and the highest +PV (80%) (Table 1).
Pair-wise comparisons between the AUC of different caries detection modalities revealed statistically non-significant differences among all modalities.
With respect to the diagnostic accuracy measures and ROC curve analysis for the determination of caries extension into the enamel or the dentin of different modalities, conventional radiography (60 kVp) showed the highest sensitivity (75%). Conventional radiography (70 kVp) showed the highest specificity (95.5%), the highest +PV (97.1%), the highest diagnostic accuracy (83%), and the highest AUC (0.831) (Table 2).
Pair-wise comparisons between the AUC of different modalities in the determination of the caries extension into the enamel or the dentin revealed statistically nonsignificant differences between all modalities.
With respect to the diagnostic accuracy measures and ROC curve analysis for the detection of incipient caries, all modalities showed the same sensitivity (90%). Digital radiography (70 kVp) showed the highest specificity (70%), the highest +PV (33.3%), and the highest -PV (97.7%). Conventional radiography (60 kVp) showed the highest diagnostic accuracy (81%) and the highest AUC (0.805) (Table 3).
With respect to the diagnostic accuracy measures and ROC curve analysis for the detection of moderate caries, conventional radiography (70 kVp) showed the highest sensitivity (91.7%), the highest -PV (97.6%), the highest diagnostic accuracy (83%), and the highest AUC (0.831). Digital radiography (70 kVp) showed the highest specificity (77.6%) and the highest +PV (40.9%) (Table 3).
With respect to the diagnostic accuracy measures and ROC curve analysis for the detection of advanced caries, all modalities showed a sensitivity of 100%. Digital radiography (60 kVp) showed the highest specificity (48.1%), the highest +PV (40%), the highest diagnostic accuracy (69%), and the highest AUC (0.688). All modalities showed the same -PV (100%) (Table 4).
With respect to the diagnostic accuracy measures and ROC curve analysis for the detection of severe caries, conventional radiography (70 kVp) showed the highest sensitivity (96.7%), the highest -PV (97.1%), the highest diagnostic accuracy (96%), and the highest AUC (0.962). Conventional radiography (60 kVp), digital radiography (60 kVp), and digital radiography (70 kVp) showed the highest specificity (100%) and the highest +PV (100%) (Table 4).
Pair-wise comparisons between the AUC of different modalities in the determination of caries severity revealed statistically non-significant differences among all modalities.
The Kappa statistic showed an inter-observer agreement of 0.754, 0.780, 0.797, and 0771 for conventional radiography (60 kVp), conventional radiography (70 kVp), digital radiography (60 kVp), and digital radiography (70 kVp), respectively. Further, the intra-observer agreement ranged from 0.765 to 0.790 for conventional radiography (60 kVp), from 0.790 to 0.814 for conventional radiography (70 kVp), from 0.800 to 0.850 for digital radiography (60 kVp), and from 0.774 to 0.786 for digital radiography (70 kVp) (Table 5).
Discussion
Upon analyzing the results of the current study, no statistically significant difference in the diagnostic accuracy for the assessment of dental caries in either conventional or digital images could be detected between 60 kVp and 70 kVp. This finding is in contrast to the following statement: "Images with a high contrast are more accurate in caries assessment than those with a low contrast." This concept, which is stated in textbooks, has been applied in many dental faculties where the oral radiology curricula are based on such textbooks.24,25,26,27 Moreover, some current intraoral X-ray machines allow changing the kilovoltage peak between 60 kVp and 70 kVp, or even between 60 kVp, 65 kVp, and 70 kVp; this option may be partially attributed to the previously mentioned statements about the relationship between short grayscale and caries detection.
When dealing with the assessment of dental caries, sensitivity and specificity as well as positive and negative predictive values have an equivalent diagnostic status. This is because it is important to detect carious lesions in affected teeth as well as to exclude caries in sound teeth. This diagnostic importance is attributed to the fact that false negative cases will lead to the progression of caries, particularly dentine caries, deeper in the tooth with a subsequent more aggressive treatment. Moreover, false positive cases will lead to unrequired restorative intervention. Therefore, it is more practical to deal with the diagnostic accuracy as a whole than dealing with each measure separately.
The results of the current study revealed that the difference between the lower and the higher kilovoltage with respect to the diagnostic accuracy was minor and non-statistically significant. As for conventional radiography, the use of 60 kVp revealed higher values in the detection of caries and the determination of caries severity in incipient and advanced caries, while the use of 70 kVp showed higher values in the determination of caries extension into the dentin and the determination of caries severity in the cases of moderate and severe caries.
The insignificant importance of changing the kilovoltage values was also evident in digital images but in a different way. The use of 60 kVp showed higher values in the determination of caries extension as well as the severity of moderate, advanced, and severe caries, while the use of 70 kVp aided in caries detection and the determination of its severity in the incipient cases.
These fluctuating results of the high and the low kilovoltage in conventional and digital radiography reflect that changing the tube potential is no longer an influencing factor in caries assessment, the concept that was valid previously on the basis of old studies.29,30 This finding is not confined to the detection of caries but extends to the determination of caries extension into the enamel and the dentin as well as the severity of the caries.
The non-significant difference between both the investigated kilovoltage peaks in the conventional radiographs may be attributed to the advances in the manufacturing of radiographic films, namely the production of films with a higher film latitude than that of the films produced in the previous decades. In the same manner, the wide dynamic range of digital systems, particularly that of photostimulable phosphor systems, may be the cause for similar results, where a high film latitude and a wide dynamic range permit obtaining diagnostically accepted images with a wide range of exposure time. Based on the fact that the exposure time is the main factor that influences the image density, which will subsequently affect the final contrast of the image, the effect of changing the tube voltage as the master factor determining the image contrast may not be a crucial one.
The results of the current study are consistent with those of Bottenberg et al,31 who used a charge-coupled device (CCD) and a complementary metal-oxide semiconductor (CMOS) instead of a PSP, which meant that the non-significant difference in caries assessment between 60 kVp and 70 kVp was not confined only to PSP systems but was also observed in solid-state systems besides conventional radiography.30,32 The results of previous studies were heterogonous to some extent either because of the use of a non-common kilovoltage33 or because of the use of the kilovoltage that is not used in intraoral radiography anymore.34
Good-to-very good inter-observer and intra-observer agreements for 60 kVp and 70 kVp in both conventional and digital radiography reflected the comparable reliability of both the investigated potentials in the caries assessment. Moreover, the small differences in agreement were not consistent among the study modalities.
In conclusion, the difference between 60 kVp and 70 kVp was not statistically significant with respect to the overall diagnostic accuracy in the dental caries assessment. Moreover, the sensitivity and the specificity as well as the positive predictive value and the negative predictive value in the considered cases were comparable and not constant for either of them in the detection of caries and the determination of its extension into the dentin or its severity. Therefore, from a clinical point of view, changing the tube voltage of intraoral X-ray machines between 60 kVp and 70 kVp has no significant effect on the accuracy of the dental caries assessment, and this lack of effect could exist in both conventional and digital radiography.






 XML Download
XML Download