

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Many times head and neck lymphadenopathy may be caused by lymphomas.1 Extranodal lymphomas are seen almost exclusively as non-Hodgkin's lymphoma (NHL) and these constitute 10-20% of all lymphomas.2 Adult NHLs commonly arise from B cells. Swelling of unknown origin presenting as NHL of the head and neck may prove to be a challenge for diagnosis.1 Salivary gland lymphomas are quite rare and the majority of them originate from B cells.3 This report described a case of 73-year-old female manifested as having both nodal and extranodal involvement, but on imaging it was shown to involve Waldeyer's ring and the larynx, orbit, spleen, and liver.
Case Report
A 73-year-old Indian female patient presented with rapidly progressive painless swelling of face, mainly localized in the parotid and submandibular region bilaterally for the duration of one year. The patient had a history of fever for the most recent two months, with unexplained weight loss (weight at the time of presentation was 35 kg). She had also noticed a recent change in her voice.
Physical examination revealed the patient to be moderately built and poorly nourished with signs of anemia. Ocular examination showed bilateral subconjuctival hemorrhage and puffiness of the eyelids. The spleen was also palpable 10 cm below the costal margin, whereas the liver was just barely palpable. Further systemic examination including that of the respiratory, cardiac, and central nervous systems was normal.
Extraorally, she had a diffuse firm swelling of both the parotid and submandibular glands (Fig. 1A), and a rubbery consistency of the cervical lymph nodes along with those of the submental, submandibular, and jugulodiagastric groups.
Intraorally, two soft, non-tender swellings of about 2×3 cm were seen in the buccal vestibule in the region of the left upper and lower second molar. Multiple nodules were also palpable in the buccal mucosa bilaterally (Fig. 1B). A routine hemogram showed pancytopenia with a hemoglobin level of 8.8 gm/dL, a total leukocyte count of 2.5×103/mm3 and platelet count of 1.03×103/µL. A lactate dehydrogenase level of 621 IU/L was noted and tests for human immunodeficiency virus (HIV) I and II were found to be non-reactive. Bone marrow cytology revealed an interstitial pattern of marrow involvement.
Panoramic and chest radiographs were unremarkable. High resolution ultrasonography and color Doppler sonography studies confirmed the enlargement of the bilateral parotid and submandibular glands, and also the buccal and lingual lymph nodes (Figs. 2A and B). The cervical group of lymph nodes revealed similar enlargement of multiple nodes belonging to IA, IB, IIA, and IIB levels along with the pre- and post-auricular and supraclavicular group of lymph nodes. Ultrasonography of the abdomen confirmed the enlargement of the spleen, which measured 17 cm. The porta hepatis lymph nodes were noted for enlargement and a hypoechogenic appearance.
Contrast-enhanced computed tomography confirmed the diffuse symmetrical enlargement of the parotid and submandibular glands (Figs. 3A and B), while asymmetric thickening of the subglottic larynx and right aryepiglottic fold were evident with narrowing of the subglottic lumen. Prominent pharyngeal tonsils confirmed the involvement of Waldeyer's ring. The ocular adnexa of the left orbit were involved, presenting as a bulky lacrimal gland.
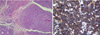
Fine needle aspiration cytology (FNAC) from the right parotid and submandibular glands, buccal vestibule, and tongue nodule showed a monomorphic population of lymphoid cells with the absence of Reed-Sternberg cells, which was suggestive of non-Hodgkin's lymphoma. Incisional biopsy of the right submandibular lymph node was performed, which revealed diffuse infiltration by sheets of a monomorphic population of moderately large cells, with moderate cytoplasm and large round vesicular nuclei having prominent nucleoli. Mitotic figures were frequently identified (Fig. 4A).
Immunohistochemistry was performed using standard techniques. The tumor cells expressed CD20 (Fig. 4B) and were immunonegative for CD10, CD3, CD5, CD23, and Cyclin D1. The Mib-1 labeling index (for proliferation marker Ki-67) was approximately 10-15%.
Diagnosis of NHL-diffuse large B-cell type was concluded based on FNAC and biopsies of the submandibular glands, parotid glands, and lymph nodes, supported by immunohistochemical positivity for CD20 marker. The patient was referred to the oncology department regarding chemotherapy and radiotherapy.
Discussion
Non-Hodgkin's lymphoma arises from a lymphocyte progenitor and comprises a heterogeneous group of highly diverse malignancies.2 25-40% of NHLs are extranodal in origin4 and usually manifest in the gastrointestinal tract, followed by the head and neck region.5 NHL mostly occurs in the pediatric age group in the head and neck region;6 however, it may be seen in an older age group, such as in the present case of a 73-year-old female.
The etiological factor for primary lymphoma of the salivary gland region is unclear.3 Oral lymphomas are frequently seen with acquired immune deficiency syndrome (AIDS). In certain individuals, it might serve as the first presentation of AIDS.7 The present case was seronegative for HIV.
The most common presentation of primary oral and paraoral lymphoma is a painless local mass with superficial ulceration.7 In the present case, patient presented with progressive painless swelling of the face involving mainly the parotid and submandibular glands. Lymphoma of the ocular adenexa is the most common in those aged over 60 years. Orbital lymphoma can involve the lacrimal gland, extraocular muscles, orbital fat, eyelids, and conjunctiva.8 In the present case, involvement of the larynx, orbit, and oropharynx were suspected based on the history and later confirmed by imaging. Based on the morphology, cell lineage, and immunohistochemical findings, the present case was categorized as aggressive NHL of diffuse large B-cell type.
To determine the prognosis and to guide therapy for NHL, staging is important. The Ann Arbor staging system9 is one of the most widely used systems, and includes physical examination, hematological tests, imaging studies, and selective biopsies.10 According to the Ann Arbor system, stage IVEB (stage IV: diffuse or disseminated foci of involvement of one or more extralymphatic organs or tissues; E: extranodal organ involvement; B: presence of systemic symptoms like fever and loss of weight) was ascribed. All IPI parameters were found to be positive in this case, thus categorizing our patient as a high risk case.
Staging of salivary gland lymphoma plays a major role in management and enables more favorable prognosis.11 NHL is associated with significant morbidity. Early stages of NHL (minimal lymph node involvement) are more manageable with a greater prospect of long-term disease-free survival, whereas advanced stages (widespread in the lymph nodes) of the disease have a lower prognostic index. Such patients are also vulnerable to infectious diseases that may involve multiple organ systems (e.g. central nervous system, liver).12
A diagnostic dilemma often occurs for oral physicians when these lymphomas occur at extranodal sites.13 The present case is disseminated NHL with predominant involvement of the salivary glands. Though the involvement of both nodal and extranodal sites was present, the patient had complained mainly of enlargement of the salivary glands. Since NHL constitutes only 1.7% of salivary gland malignancies,14 a clinical diagnosis of lymphoma is rarely suspected at initial presentation.
In conclusion, the present case emphasizes the importance of imaging and prognostic markers for staging, which is essential for management.



 XML Download
XML Download