

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Osteomas consist of dense bony proliferations of histologically normal membranous bone, which vary from slight thickening to large masses and may affect most parts of the skeleton. They are usually restricted to the craniofacial skeleton and are rare in other bones.1 The most common sites in the craniofacial region include the mandible and the paranasal sinuses.2,3 It has been suggested that most osteomas in the maxillofacial region are reactive bone hyperplasia or advanced bone ossification.4 Osteomas involving the mandibular coronoid process are rare and such tumors may be a cause of trismus.5-10 Lewars5 reported the first case in 1959, following which five more cases6-10 have been described in the literature (Table 1). The purpose of this report was to draw attention to rare but possible causes of trismus as well as to note the scarcity of the available literature on the topic.
Case Report
A 26-year-old female patient visited the Department of Oral Medicine and Radiology, Subharati Dental College complaining of gradual reduction of her mouth opening over a period of two years and associated difficulty in chewing. There was no history of trauma to the oral and maxillofacial region. The maximum mouth opening was about 20 mm with deviation of the mandible to the right side while opening (Fig. 1). Mild tenderness was noticed over the right temporomandibular joint area. On intraoral examination, a bony mass in the coronoid process could be palpated along with tenderness in the region.
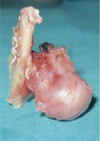
A panoramic radiograph (Vatech Inc., Hwaseong, Korea) (Fig. 2) revealed a radiopaque mass about 1.5 cm×1 cm extending from the right coronoid process. A non-contrast computed tomogram (CT/e GE, Fairfield, CT, USA) of the region revealed a bony outgrowth associated with the right coronoid process projecting anteromedially with a short and narrow stalk causing erosion of the posterolateral wall of the right maxillary sinus (Fig. 3A). A three-dimensional CT image of the region also showed the presence of a coronoid mass (Fig. 3B). Based on the clinical and radiographic findings and considering the history of slow progression, a clinical diagnosis of benign osseous neoplasm of the right mandibular coronoid process was made. Under general anaesthesia, using an intraoral approach, excision of the mass along with the coronoid process was performed. The surgical specimen comprised a mushroomshaped bony mass measuring around 2.5 cm×3 cm×3 cm in size (Fig. 4). On microscopic examination, the specimen revealed a highly cellular collagenized stroma with abundant interconnected bony trabeculae (Fig. 5A). Higher magnification revealed cancellous lamellated bony trabeculae with lacunae containing osteocytes with osteoblastic rimming (Fig. 5B). Based on these features, the final diagnosis of osteoma of the right mandibular coronoid was made, and the patient was advised to perform mouth opening exercises and physiotherapy. The post-operative recovery of the patient was satisfactory and the patient could open her mouth up to 35 mm after one month and one year of follow-up (Fig. 6). The two-year follow-up of the patient showed no signs of recurrence following surgery.
Discussion
Osteoma is a benign osteogenic tumor arising from the proliferation of the cancellous or compact bone. It can be of a central, peripheral, or extra-skeletal type.11 A central osteoma arises from the endosteum, a peripheral one from the periosteum, and an extra-skeletal soft tissue osteoma usually develops within the muscle.12 The present case represented the peripheral and cancellous variant of osteoma arising from the periosteum.
Many tumors and conditions involving the coronoid process may result in trismus. Other similar lesions in the region may include osteochondroma, osteoid osteoma, osteoblastoma, coronoid hyperplasia, and osteosarcoma.
Osteochondroma is the most common benign neoplasm of the skeleton, and more than 15 cases of osteochondroma involving the coronoid process have been reported in the literature.13,14 A coronoid osteochondroma can also present as a progressive painless mass that causes progressive reduction in the mouth opening.13 Differentiation between osteoma and osteochondroma can be made radiographically and histopathologically on the basis of the presence of a cartilaginous cap.
Osteoblastoma is a benign neoplasm of the bone arising from the osteoblasts and has also been reported to affect the coronoid process.15,16 However, pain and swelling, which are the main presenting features were absent in our case. Radiographically, the lesion may often have a soft tissue capsule around the periphery indicating that the tumor is more mature in the centre and the internal structure is more radiolucent as compared to osteoma.17 Histopathologically, the presence of multinucleated giant cells and more vascularisation helps to differentiate it from an osteoma.15,16
Osteoid osteoma can be differentiated from osteoma on the grounds of nocturnal pain relieved by NSAIDs, radiographic features showing a nidus of osteoid tissue surrounded by densely reactive bone.1
Absence of rapidly progressing swelling, tenderness, erythema of the overlying mucosa, anesthesia, paresthesia clinically, and absence of ill-defined borders with a typical sunray or hair-on-end appearance could lead to ruling out the possibility of osteogenic sarcoma or osteosarcoma.
Coronoid osteomas are asymptomatic and cause painless swelling until their size and position interferes with functioning.5,6 They can occur at any age but are more frequently found in young adults and men. Our case was of a 26-year-old female patient who was initially asymptomatic but gradually developed deviation of the mandible towards the right side, which was associated with mild tenderness of the right temporomandibular joint.
The first reported case of osteoma involving the mandibular coronoid process was described by Lewars5 in 1959, following which five more cases of coronoid osteoma have been reported; however, additional cases may have gone unreported. To the best of our knowledge, our case is the seventh case of osteoma involving the coronoid process reported in the literature, and has been diagnosed based on its clinical features, and conventional and digital radiographs followed by histopathologic examination. An association of our case with Gardner's syndrome was not found.
Surgical excision is the treatment of choice in patients with functional hindrance and recurrence has not been reported.6,10 This case was also managed by surgical excision, and there were no signs of recurrence after 2 years of follow-up.
The present report, therefore, was an attempt to draw the attention of diagnosticians to this rare case of coronoid osteoma, as it might be one of the possible causes of progressive asymptomatic reduction of mouth opening; to review the available literature; and to emphasize the good prognosis of the condition if diagnosed and managed properly. In addition, adequate clinical examination and use of proper imaging modalities in diagnosing unusual conditions affecting the temporomandibular joint may also be needed.18






 XML Download
XML Download