

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A dentigerous cyst is defined as a cyst that originates by the separation of the follicle from around the crown of an unerupted tooth and is attached to the tooth at the cementoenamel junction.1-6 Therefore, if pericoronal unilocular cystic radiolucency is associated with a tooth crown not developed to form the cemento-enamel junction yet, and the underdeveloped crown may be floating within the radiolucency, the provisional diagnosis might be odontogenic keratocyst rather than dentigerous cyst. This is because the suspected odontogenic keratocyst has presumably arisen from dental lamina rests near an unerupted tooth and has grown to envelop the unerupted tooth.7 The author experienced 8 cases of pericoronal radiolucency involving incomplete crowns that had odontogenic keratocysts as the first impression, but half of them turned out to be dentigerous cysts histopathologically. There has been no report concerning odontogenic cysts involving an incompletely developed crown. The purpose of this report was to show that dentigerous cysts might develop before the completion of the cemento-enamel junction of the developing crown.
Case Report
Case 1
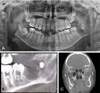
A 7-year-old female patient was referred from a private dental clinic to evaluate a pericoronal radiolucency at the right lower molar region. On clinical examination, there was no sign of swelling or infection. A panoramic radiograph revealed a well-defined round unilocular radiolucency touching the developing crown of the right lower second molar, which was displaced downwardly. The cemento-enamel junction of the involved tooth was incomplete (Fig. 1A). The CBCT images showed bucco-lingually expanded cortical plates associated with the lesion and a mandibular canal displaced toward the inferior cortex (Fig. 1B-E). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised but the tooth was preserved. The histopathological diagnosis proved to be an odontogenic keratocyst. The 6-month follow-up panoramic radiograph showed uneventful healing of the lesion with upward movement of the more developed lower right second molar (Fig. 1F).
Case 2
A 12-year-old female patient was referred from a private dental clinic for evaluation of a cystic lesion in the left mandibular posterior region. On clinical examination, there was a swelling of the left mandible that was hard to the touch, but the pain and soft tissue swelling, which was the initial chief complaint of the patient, had subsided after the administration of antibiotics for several weeks. A panoramic radiograph revealed a well-defined round unilocular radiolucency surrounding the developing crown of the left lower third molar which had not developed to the cementoenamel junction yet (Fig. 2A). The CBCT images showed a lingually expanded cortical plate associated with the lesion, but the buccal cortical plate was perforated. The mandibular canal was identified inferior and lingual to the lesion (Fig. 2B-E). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with the extraction of the involved tooth. The histopathological diagnosis proved to be an odontogenic keratocyst with chronic inflammation and a foreign body reaction, and the cyst wall showed periosteum adhesion.
Case 3
A 12-year-old female patient was referred from a private dental clinic for evaluation of a cystic lesion at the right mandibular posterior region. On clinical examination, there were no specific symptoms, but the patient complained of having had a pus taste for the previous 6 months. A panoramic radiograph revealed a well-defined round unilocular radiolucency surrounding the transversely positioned crown of the lower right third molar (Fig. 3A). The CBCT images showed a bucco-lingually expanded cystic lesion associated with the buccally displaced, developing right lower third molar, but the cemento-enamel junction of the crown was incomplete. The mandibular canal was displaced downward due to the lesion (Fig. 3B-D). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with the extraction of the involved tooth. The histopathological diagnosis proved to be an odontogenic keratocyst.
Case 4
A 12-year-old female patient was referred from a private dental clinic for the evaluation of a cystic lesion at the left mandibular ramus region. On clinical examination, there was a moderately painful swelling of the left mandibular angle area. The pain had started 2 weeks earlier, and mouth opening was limited. A panoramic radiograph revealed a large well-defined round unilocular radiolucency surrounding the developing crown of the lower left third molar, which was displaced upward to the sigmoid notch. The cemento-enamel junction of the involved tooth was incomplete (Fig. 4A). The CBCT images showed a bucco-lingually expanded cortical plate associated with the lesion that surrounded the underdeveloped crown of the left lower third molar. The mandibular canal was identified inferior and lingual to the lesion (Fig. 4B-C). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with the extraction of the involved tooth. The histopathological diagnosis proved to be an odontogenic keratocyst.
Case 5
A 6-year-old female patient was referred from a private dental clinic to evaluate the swelling at the left lower posterior region. On clinical examination, there was a 1-month duration of swelling of the left lower molar region. The patient's systemic medical history included unspecified thrombocytopenia and a bleeding tendency. A panoramic radiograph revealed multiple bilateral radiolucencies of the mandible and another separate well-defined round radiolucency involving the developing crown of the lower left second molar (Fig. 5A). The left mandibular multilocular radiolucency involving the left lower second primary molar, the lower part of the developing premolars, and the mesial part of the lower left first molar had been operated on 1 year earlier, and the lesion was a giant cell granuloma. This time the unilocular cystic radiolucency-associated developing crown of the left lower second molar was to be managed. The cemento-enamel junction of the involved tooth was incomplete. The CBCT images showed bucco-lingually expanded cortical plates associated with the lesion and the mandibular canal was displaced inferiorly and lingually (Fig. 5B-D). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with removal of the developing lower left second molar after platelet transfusion. The histopathological diagnosis proved to be a dentigerous cyst.
Case 6
A 9-year-old male patient was referred from a private dental clinic for evaluation of a hard mass in the left mandibular angle region. On clinical examination, there was a painful swelling of the left mandibular angle. The pain and swelling had first been noticed 1 year earlier, but only medication was applied, and then pus drainage through the gingival swelling of the lower left first and second molar area had been started 1 month before presentation to our clinic. A panoramic radiograph revealed a well-defined round unilocular radiolucency surrounding the developing crown of the lower left third molar, which was displaced distally to the mandibular ramus, and the cemento-enamel junction of the tooth was incomplete (Fig. 6A). The CBCT images showed a bucco-lingually expanded cortical plate associated with the lesion, which surrounded the underdeveloped crown of the lower left third molar (Fig. 6B-C). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with the extraction of the involved tooth. The histopathological diagnosis proved to be a dentigerous cyst.
Case 7
A 12-year-old male patient was referred from a private dental clinic to evaluate a cystic lesion at the left mandibular posterior region. On clinical examination, there was a painful mild swelling of the left mandibular angle area. The pain and swelling had started 3 days earlier but had subsided somewhat after the medication. A panoramic radiograph revealed a well-defined round unilocular radiolucency surrounding the developing crown of the left lower third molar without completion of the cemento-enamel junction (Fig. 7A). The CBCT images showed a well-defined round radiolucency with no cortical expansion surrounding the underdeveloped crown of the lower left third molar. The mandibular canal was identified inferior and lingual to the lesion (Fig. 7B-C). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with the extraction of the involved tooth. The histopathological diagnosis proved to be a dentigerous cyst.
Case 8
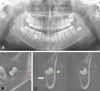
A 12-year-old male patient was referred from a private dental clinic for evaluation of a cystic lesion at the left mandibular posterior region. On clinical examination, there was a painful mild swelling of the left mandibular angle area. The pain and swelling had started 1 week earlier but had subsided after medication was administered. A panoramic radiograph revealed a well-defined round unilocular radiolucency surrounding the crown of the left lower third molar before the completion of the cemento-enamel junction (Fig. 8A). CBCT images showed a well-defined round radiolucency with no cortical expansion surrounding the underdeveloped crown of a lower left third molar. The mandibular canal was identified inferior and lingual to the lesion (Fig. 8B-D). A provisional diagnosis of odontogenic keratocyst was made, and the lesion was excised with the extraction of the involved tooth. The histopathological examination showed flattened squamous epithelium and inflamed stroma showing extensive odontogenic epithelial remnants, consistent with a dentigerous cyst.
Discussion
The differential diagnosis of Darling et al6 for a uniloular pericoronal radiolucent lesion of the posterior mandible included common lesions such as the dentigerous cyst and the odontogenic keratocyst (keratocystic odontogenic tumor), along with less common lesions including the glandular odontogenic cyst, ameloblastoma, adenomatoid odontogenic tumor, ameloblastic fibroma, central odontogenic fibroma, desmoplastic fibroma, squamous cell carcinoma arising in a dentigerous cyst, and a metastatic lesion to the jaw. Curran et al8 reported actual pathological results of their 2,646 pericoronal lesions in adults (18 years and older) submitted to an oral and maxillofacial pathology biopsy service. Of the 2,646 lesions, 1,776 (67.1%) were diagnosed as follicular tissue. The pathologically significant lesions totaled 872 (29.1%). Among the 872 lesions, the diagnoses included 673 dentigerous cysts with an additional 79 dentigerous cysts with mucous cell prosoplasia, 71 odontogenic keratocysts, 19 odontomas, 13 ameloblastomas, 6 calcifying odontogenic cysts, 6 carcinomas, 4 calcifying epithelial odontogenic tumors, and 1 odontogenic myxoma.
Therefore, the most reasonable provisional diagnosis of well-defined unilocular pericoronal radiolucency might be the dentigerous cyst, but for these reported cases, odontogenic keratocysts were chosen because of the incompleted cemento-enamel junction of the involved tooth.
The odontogenic keratocyst arises from cell rests of the dental lamina and their growth may be related to unknown factors inherent in the epithelium itself or enzymatic activity in the fibrous wall.7 An unerupted tooth is involved in the lesion in 25% to 40% of cases; in such instances, the radiographic features suggest the diagnosis of dentigerous cyst.7,9 In such cases, the cyst has presumably arisen from dental lamina rests near an unerupted tooth and has grown to envelop the unerupted tooth.7 These are often called follicular odontogenic keratocysts.10 However, even in the cases of follicular odontogenic keratocyst, the associated crown of the involved tooth has a complete crown with a cemento-enamel junction and has the appearance of a dentigerous cyst.10-12 The 8 cases reported in this study were therefore quite challenging to diagnose, showing not only odontogenic keratocysts but also dentigerous cysts that may develop before the completion of the crowns. The pathogenesis of dentigerous cyst is uncertain, but apparently it develops by accumulation of fluid between the reduced enamel epithelium and the tooth crown.1 The patients of this report are young, and this may explain how the fluid accumulation could occur before the completion of the cemento-enamel junction.






 XML Download
XML Download