

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Prediction of bone quality is very important for evaluating the healing phase after bone fracture, the load-bearing potential after installation of an implant, and the bone change around a pathologic lesion. Therefore, many studies on the parameters predicting bone quality have been performed. The term 'bone quality' has been used ambiguously. The best known bone quality classification in dentistry was proposed by Lekholm and Zarb.1 They classified the bone quality based on both morphology and the proportion of cortical and trabecular bone. This classification has been used widely in clinical practice up to the present; however, the efficacy of the determination of bone types has not yet been scientifically validated.2
Recently, mechanical strength has been accepted as an indicator of bone quality in general. Several studies have reported that, in addition to bone mass, structural architecture also provided a useful predictor of mechanical strength.3-5 Some other approaches used to assess bone quality include evaluation of bone mineral density,6,7 histologic structure,8 and histomorphometric analysis.9 These methods had limitations in evaluating the mechanical properties of bone in a subjective or quantitative manner.10
Several studies have reported on the variations in the quality and quantity of jaw bone according to the success rate of implant installation at different jaw sites.11 Most of these studies have emphasized the role of cortical bone for achieving primary stabilization due to its stiffness. However, mechanical characteristics of trabecular bone also influence the load-bearing capacity of the implant-bone union while the greater part of the fixture is in contact with trabecular bone. Few studies have investigated the features of maxillary and mandibular trabecular bone, especially their mechanical behavior.12 A number of studies have been published to demonstrate various features in jaw trabeculation;13,14 however, the three-dimensional (3D) microstructures specific to the maxilla and mandible have not been clearly described.
High resolution scanning by micro-computed tomography (micro-CT) was developed in the late 1990s to image tiny specimens with resolutions as small as a micrometer. This made it possible to assess the trabecular architecture in order to estimate the mechanical properties of bone using specific parameters in three dimensions with micro-CT.15
The purpose of this study was to analyze human maxillary and mandibular trabecular bone with 3D microstructure data acquired with micro-CT, and to characterize site-specific variations in trabecular microstructure.
Materials and Methods
Bone specimens
Four sets of dry human jaw bone were prepared. The protocol for this study was approved by the institutional ethics committee of the associated institution.
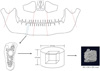
Using a micro-cutting and grinding system, the 300 CP precision parallel-control Exakt (Apparatebau GmbH, Norderstedt, Germany), the mandibles and maxillae were cut para-sagittally into consecutive slices 4 mm thick in an approximately perpendicular direction to the occlusal plane under continuous water irrigation. Cylindrical specimens that included trabecular bone only were harvested from each sectioned plate using a trephine bur with a 4.9-mm internal diameter.
The regions were categorized as follows:
Anterior maxilla (AX): including the incisors to the distal aspect of the canines (n=10)
Posterior maxilla (PX): from the premolar to the maxillary tuberosity (n=18)
Anterior mandible (AN): including the incisors to the distal aspect of the canines (n=6)
Posterior mandible (PN): from the premolar to the mandibular angle (n=23)
Condyle (C): above the sigmoid notch (n=12)
A total of 69 bone samples was obtained and grouped by each region. Figure 1 illustrates the procedures of this study.
Micro-CT
The micro-CT examination of each bone specimen was performed using a SkyScan 1172 (Skyscan, Antwerp, Belgium). The specimen was placed on the holder between the X-ray source and the CCD camera, such that the whole specimen was encompassed in the field of view. The exposure conditions were 192° rotation with 0.4° rotation step, 0.5-mm aluminum filtration, 80 kVp, 100 µA, and 19.57-µm pixel. During image acquisition, the bone specimens were kept moist with wet tissue in water. The projection data were then reconstructed with NRecon (ver. 1.5.1.3, Skyscan, Antwerp, Belgium) to create 3D images. The volume of interest (VOI) was 3.91 mm×3.91 mm×3.91 mm with a 202 pixel ×202 pixel×202 pixel cube in the cylindrical bone specimens. The images were processed using a fixed threshold value of 193 to separate the trabecular bone from the marrow spaces. Threshold was determined as the value of both CT and binary image presenting minimal difference in trabecular portion.
Examples of the 3D reconstructed model from each site are shown in Figure 2. The procedures were performed by Skyscan™ CT analyzer software (CTAn version 1.7, Skyscan, Antwerpen, Belgium).
Three-dimensional image analysis
From each VOI, the following structural parameters were determined: the percent bone volume (BV/TV), bone specific surface (BS/BV), trabecular thickness (Tb.Th), trabecular separation (Tb.Sp), trabecular number (Tb.N), structure model index (SMI), and degrees of anisotropy (DA). The 3D parameters were calculated by SkyScan™ CT analyzer software.
Statistical analysis
The mean value and standard deviation of each parameter was calculated for 4 groups (AX, PX, AN, PN) excluding the condyle group. The values were compared by the analysis of variance (ANOVA). Tukey's multiple comparison test was used to determine whether significant differences existed in the measured parameters in between the regions (at a 95% confidence interval level, α=0.05).
A t test was carried out to compare the parameters of the mandibular body area (N=AN+PN) and the mandibular condyle (C). IBM SPSS Statistics (version 21, SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
Comparison of 3D microstructural parameters among the regions
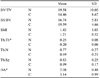
Table 1 demonstrates the values of the parameters measured in the various sites other than the mandibular condyle. ANOVA indicated that there were significant differences between the groups (P<0.05) for the BS/BV, Tb.Th, and DA parameters. Notably, the BS/BV was the highest at the PX and the lowest at the AN (Fig. 3). The difference between these two groups was statistically significant (P=0.033).
One of the structural parameters, Tb.Th, ranged from 0.12 mm to 0.41 mm and showed significant differences between groups (P=0.002). The highest value was measured at the AN and the lowest at the PX. The groups showing significant differences are marked in Figure 4.
BV/TV revealed a wide range of values from 6.75% to 48.92%. Even though there was no statistical significance, the anterior regions showed a higher BV/TV value than the posterior region, and the mandibular region had higher value than the maxillary regions (Fig. 5). This tendency toward a difference was similar to that of Tb.Th, and opposed to that of BS/BV. No significant differences were observed in Tb.Sp, Tb.N, or SMI. Tb.Sp ranged from 0.44 mm to 1.77 mm; however, there was little to no difference between groups (P=0.533). The Tb.N, which ranged from 0.34 to 1.73, was lowest at the AN. DA was lowest at the AN and highest at the PN.
Tukey's test (α=0.05) revealed that the AN region had a significantly higher Tb.Th value compared with the other regions, but the difference did not attain statistical significance for BV/TV, Tb.Sp, Tb.N, or SMI. The differences in the values from the trabecular bone of each region were not significant, except for Tb.Th and BS/BV, which were highest in the AN (Table 2).
Comparison of 3D microstructural parameters between the mandibular body and mandibular condyle
A t-test revealed differences between the mandibular body and mandibular condyle for the Tb.Th and DA parameters (P=0.032, P=0.002, respectively). The Tb.Th was higher in the mandibular body than the mandibular condyle, and the DA was higher in the mandibular condyle than the mandibular body (Table 3).
Discussion
Bone quality is considered to be a predictor of implant success; however, the parameters for evaluating bone quality have not been clearly established. There have been many attempts to propose classifications of bone quality. Lekholm and Zarb proposed a classification based on the macrostructure of the morphology and distribution of both cortical and trabecular bone,1 and Jensen proposed a classification correlated with the anatomic site.16 Misch et al proposed a density-related macrostructure bone classification using subjective tactile sensation during bone drilling,12 and Friberg et al used an objective cutting resistance to predict the initial stability of an implant.17
Recently, image-based bone density evaluation by CT using the Hounsfield index was suggested.7 However, quantification of bone mass or bone density itself was not sufficient to describe the mechanical properties of bone. Riggs et al suggested that increasing the bone mass in osteoporotic patients by medication did not guarantee either an increase in bone strength or a decrease in the fracture risk.18 This study showed that bone structure was another important factor influencing the mechanical strength of bone. There have been many attempts at analyzing the trabecular structure in two-dimensional images using the fractal dimension.19,20 With the development of high-resolution imaging modalities, new methods of analyzing the microstructure in 3D images have made it possible to evaluate and predict bone quality more precisely in a noninvasive manner.
Although many studies have investigated trabecular microstructure, only a few have been conducted on human jaw bone because a high resolution scanner, particularly micro-CT, might be difficult to apply in practice, given the high exposure dose and small field of view. One report demonstrated the site-specific microstructure of the mandible and maxilla.10 However, it provided data from the maxilla and mandible of only one cadaver with one site-specific specimen from each region. Therefore, the results were unlikely to represent human bone microstructure in general.
The present study proposed microstructural parameters from specific jaw sites of the human skull. BV/TV indicated that the amount of bone was the greatest in the anterior mandible, although the difference was not statistically significant. The anterior region showed a greater BV/TV value than the posterior region, and the value was greater in the mandible than the maxilla. This tendency corresponded with Jensen's site-specific variation of bone density measured using CT scan.16 The Tb.Th value showed a similar tendency in this study. On the other hand, BS/BV, a parameter characterizing the complexity of structure, showed an inverse relationship with BV/TV. The values of Tb.N and Tb.Sp showed no significant difference between the regions; however, the tendency toward a difference in Tb. N and Tb.Sp among the jaw regions was opposite that of the study results from Fanuscu and Chang.10 Specifically, the present study demonstrated that the anterior and mandibular regions showed greater Tb.Th and Tb.Sp values, and a smaller Tb.N value, than the posterior and maxillary regions. These parameter values implied that the high bone density of the anterior mandible was due to the thick trabeculae rather than complex structure. On the other hand, Fanuscu and Chang found a greater Tb.N value with a smaller Tb.Sp value in the anterior mandible, suggesting a complex and compact structure in this region.10
The mandibular condyle has been studied as a separate part from the other jaw bone areas because the condyle has a unique trabecular structure and mechanical properties to resist strain.21,22 For that reason, we compared the 3D structural parameters of the condyle and the other regions of the mandible in this study. The values of Tb.Th and DA showed a significant difference between the mandibular condyle and other mandibular regions. The condylar region had thinner trabeculae and a higher degree of anisotropy than the mandible. A higher DA means that the trabecular bone of the mandibular condyle is structurally anisotropic, and our result was in agreement with other research results. Giesen and van Eijden found that the trabecular bone of the condyle mainly consisted of parallel plates perpendicular to the medio-lateral condylar axis.21 Anisotropy is a measure of 3D asymmetry or the presence or absence of preferential alignment of structures along a particular directional axis, and DA is one of the most important determinants of mechanical strength. It is known that the trabeculae of isotropic structures are related to increased mechanical strength since force might be evenly dispersed among them. Conversely, anisotropic structure has less resistance to external force. However, there is a more complex relationship between mechanical properties and structure. Some studies have revealed the mechanical anisotropy of the mandibular condyle and the microstructural anisotropy of condylar trabecular bone; they concluded the orientation of strain followed the direction of the applied load and the principal mechanical direction correlated significantly with the principal structural direction.23,24 Therefore, the difference in the DA value between the condyle and mandible might indicate that the directions and types of forces in each region were different. The present study had a number of possible limitations. First, the number of samples of each group was not controlled. This was due to the complicated procedure of bone specimen harvesting. We could not prepare an even number of specimens from each region because we obtained specimens composed of only trabecular bone without cortical bone or tooth structures. Second, the dentate or edentulous condition of the jaw was not considered when harvesting the bone specimens and analyzing the data. Third, there was no consideration of the microstructural difference between alveolar bone and basal bone. It has been revealed that there are physical and mechanical differences between the alveolar and basal trabecular bone.25 The stability of an implant is provided by the alveolar trabecular bone, so further research investigating the microstructural variation of the alveolar bone of specific jaw sites is needed.
To our knowledge, this was the first comprehensive study on specific jaw bone sites using 3D microstructural parameters. Despite some limitations, these results would be useful in implant planning on specific sites and as a reference for comparing the microstructure of abnormal trabecular bone caused by pathologic lesions. However, micro-CT may not be routinely applicable due to its high radiation dosage and small field of view. Further studies to analyze the microstructure of trabecular bone using clinically applicable imaging modalities are needed.
In conclusion, we analyzed and compared the 3D trabecular microarchitecture of various sites on the jaw bone. The anterior mandible had thick trabeculae and lower bone surface density; however, no specific characteristics of the microstructure at each region were identified. The mandibular condyle revealed a higher value of anisotropy. These results suggested that different mechanisms of external force might exist at the condyle than at other sites of the jaw bone.






 XML Download
XML Download