

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fusion and gemination are abnormalities in tooth development with close similarities but different etiologies.1 Owing to the difficulty in differentiating gemination from fusion, these anomalies are both commonly referred to as 'double tooth'.2
Traditional terminology classifies fusion as a union of two separately developing tooth germs typically leading to one less tooth than normal in the affected arch. Radiographically, the presence of two root canals and one or two roots may be evident.3 Gemination is the incomplete splitting of a single tooth bud resulting in a larger tooth and presenting with a normal number of teeth in the oral cavity.4 A similar condition which presents with a normal number of teeth and makes differentiation from gemination difficult is diphyodontic gemination, wherein fusion occurs between a supernumerary tooth and a normal tooth.5 Gemination is more prevalent in the anterior maxillary region, whereas fusion is more common in the anterior mandibular dentition.1
The prevalence of tooth fusion is estimated to be 0.5 to 2.5% in the primary dentition,6 whereas it is even lower in the permanent dentition.7 The prevalence of fusion between permanent and supernumerary teeth is 0.1% and usually involves maxillary anterior teeth.8 The prevalence of double tooth was found to be in 0.6% of primary dentition in a white population.9 A higher prevalence of 2.8% in primary dentition and 1.0% in permanent dentition was reported in a Japanese, Chinese, and American Indian population.10
Complex root canal morphology is a challenge for endodontic diagnosis and treatment. Owing to the limitation of conventional radiographs in assessing root canal configuration, attributable to its two dimensional representation of three dimensional structures, employment of advanced three dimensional imaging techniques has recently become invaluable. The use of high-end imaging modalities such as computed tomography (CT) can assist the clinician in making a confirmatory diagnosis and determining the treatment plan before undertaking the actual treatment.
The incidence of fusion in mandibular incisors is rare, and to the best of our knowledge, fusion of a mandibular lateral incisor with its supernumerary counterpart presenting with four root canals has not been reported. Therefore, the aim of this report is to present the endodontic management of an unusual case of "double tooth" in relation to a left mandibular lateral incisor exhibiting four root canals, diagnosed with the aid of 64-slice multidetector computed tomography (MDCT) scanner.
Case Report
A 17-year-old female was referred to the Department of Endodontics for the treatment of the left mandibular lateral incisor. Root canal treatment had been initiated by a general practitioner for the tooth in question two months before. Clinical examination of the tooth revealed a discolored crown with an increased mesiodistal width (Fig. 1A) which elicited slight tenderness on percussion. The number of teeth in the arch was normal.
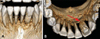
An intraoral periapical radiograph revealed the presence of multiple root canals of the tooth in a single wide root with diffuse periapical radiolucency (Fig. 2A). Subsequent to obtaining informed consent from the patient, three-dimensional (3D) imaging using 64-slice MDCT scanner (Brilliance CT 64-channel, Philips Healthcare, Andover, MA, USA) was planned in order to confirm the morphology of the complex pulp space. An MDCT scan of the mandible was performed and images were acquired using dental software program DentaScan (GE Healthcare, Milwaukee, WI, USA). In addition to the increased mesiodistal width, 3D reconstructions disclosed a lingual radicular groove in relation to the left mandibular lateral incisor (Fig. 3). The axial view revealed three canals at the cervical level: large distal, mesial, and middle canals (Fig. 4A). At the junction of the cervical and middle third, the middle canal merged with the division of the distal canal. An axial slice at the middle third of the root revealed two distal canals and a single mesial canal with a narrow isthmus joining all of the three canals (Figs. 4B and C). A curved coronal image showed the presence of a large distal and a mesial canal (Fig. 5A). Another coronal image confirmed that the distal canal divided into two separate canals (Fig. 5B). A communication between the mesial and distal canals was also evident (Fig. 5C). With the help of the axial and coronal images of MDCT, it could be assumed that the left mandibular lateral incisor, which had a single canal, was fused with a supernumerary tooth distal to it, which had two root canals. The fourth canal might have represented a connection between the root canal systems of the fused teeth. A sagittal image confirmed the presence of aberrant root canal morphology and presence of a large periapical radiolucency (Fig. 6).
Under local anesthesia administration and rubber dam isolation, an access opening was refined using an EX 24 bur (Mani, Tochigi, Japan), revealing an unusually large pulp chamber. On pulp chamber exploration, a perforation was detected on the labial surface of the tooth near the cement-enamel junction, which was immediately sealed using flowable resin (Filtek flow; 3M ESPE, St Paul, MN, USA). Three separate orifices of the mesial, middle, and distal canals were located (Fig. 1B) with the distal canal further dividing into two separate canals. The working length was determined with the help of an apex locator (Root ZX, Morita, Tokyo, Japan), which was later confirmed with a radiograph (Fig. 2B).
Biomechanical preparation was then carried out employing Protaper™ hand instruments (Dentsply Maillefer, Ballaigues, Switzerland) under copious irrigation with 2.5% sodium hypochlorite (KMC Pharmacy, Manipal, India) and 17% ethylenediaminetetraacetic acid (EDTA) (Merck, Dermstadt, Germany). Calcium hydroxide (Ultracal XS, Ultradent, South Jordan, UT, USA) was placed in the root canals, and the access cavity was temporized with Cavit G (3M ESPE, Seefeld, Germany). Thereafter, calcium hydroxide dressing was renewed twice at an interval of two weeks between each appointment following which the tooth was completely asymptomatic. The root canals were obturated by cold lateral compaction of gutta-percha using a zinc oxide eugenol sealer (Kemdent, Associated Dental Products Ltd., Wiltshire, UK) (Fig. 2C) and the access cavity was restored with composite resin (3M ESPE Dental Products, St. Paul, MN, USA). A one year follow-up radiograph showed satisfactory healing of the periapical lesion (Fig. 2D).
Discussion
Although there have been many studies on the occurrence of double tooth, there is still much discussion concerning the nomenclature. Some authors have tried to differentiate them by counting the teeth11 or by observing the root morphology,12 and others have described fusion and gemination as synonyms.13 Some authors simply called the phenomenon double teeth,14 double formations, joined teeth,2 fused teeth,15 or dental twinning4 to avoid confusion over terminology.
Cases of double tooth in relation to mandibular lateral incisors have been reported,1,16,17 but our case was unique, as the fused mandibular lateral incisor presented with four root canals and we confirmed the complex root canal anatomy using MDCT. After a thorough review of the literature and conducting a PubMed search using the keywords "double tooth", "fusion", or "mandibular incisor", we did not come across any report of a fused mandibular lateral incisor exhibiting four root canals. There was a similar case report of a fused mandibular lateral incisor: however it presented with three root canals.17
Although the anomaly in this present case most probably represents a fusion of a lateral incisor with a supernumerary tooth based on Mader's two tooth rule,18 we prefer to use the terminology "double tooth" to avoid confusion. Mader's two tooth rule states that (1) If the fused teeth were counted as two teeth and the number of teeth in the dental arch was normal then it can be considered to be a case of fusion. (2) When the abnormal dental structure was counted as two teeth and an extra tooth was present in the dental arch then it can be considered a case of gemination or a case of fusion between a normal and supernumerary tooth. It is noteworthy that supernumerary teeth are not uncommon; they appear in 0.3 to 3.8 percent of the population.19 However, the exact differentiation between fusion and gemination might not be critically important with respect to their treatment.
Lyroudia et al20 focused on the importance of familiarity with root canal morphology before endodontic treatment, especially in complicated cases. The use of MDCT in this unusual case greatly contributed towards making a confirmatory diagnosis and nonsurgical endodontic management. From the MDCT images, it could be assumed that the left lateral incisor, which had a single canal (Vertucci's type I canal morphology), might have fused with a supernumerary tooth present distal to it. The supernumerary tooth might have exhibited Vertucci's type III canal morphology (Fig. 7). Since the middle canal was negotiable up to the junction of the cervical and middle third, there was a possibility that it might be a communication between the root canal systems of the fused teeth. It was noteworthy that communications between the root canal systems of fused teeth have been well documented in the literature.21
Three-dimensional imaging is now becoming the standard of care for dental radiography. While two-dimensional conventional radiographic images still has a place in a dental practice, many patients need more for optimal care. Better preoperative assessment and understanding of pathology when using MDCT makes treatment planning easier and more accurate. The case illustrated in this report emphasizes the need for accurate diagnosis based on a comprehensive evaluation using all diagnostic modalities available, including 3D digital imaging techniques.
The most important advantage of 3D imaging in endodontics is that it demonstrates anatomic features in three dimensions that intraoral and panoramic images cannot. MDCT units reconstruct the projection data to provide inter-relational images in three orthogonal planes (axial, sagittal, and coronal). Root morphology can be visualized in 3D, as can the number of root canals and whether they converge or diverge from each other. Unidentified and untreated root canals may be identified using axial slices, which may not be readily identifiable with periapical radiographs.
To conclude, as double tooth is a rare malformation, dental practitioners should be prepared to meet unusual chamber and canal morphology when performing root canal treatment. Proper diagnosis and treatment planning for endodontic management of such teeth by using conventional and advanced three dimensional imaging techniques can ensure predictable and successful results.






 XML Download
XML Download