

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The styloid process is a cylindrical, long cartilaginous bone located on the temporal bone. The term, "elongated styloid process", was first defined by Eagle in 1937.1 The normal size of the styloid process varies significantly, approximately 20-30 mm.2,3 The styloid process elongation can be assumed when either the styloid process or the adjacent stylohyoid ligament ossification shows an overall length greater than 30 mm2,4 or 45 mm.5
Patients are usually asymptomatic, while 4% of them present symptoms.6 The calcified stylohyoid ligament and elongated styloid process can result in several symptoms associated with syndromes such as the classical Eagle syndrome, carotid artery syndrome, stylohyoid syndrome, and pseudostylohyoid syndrome.7 Only when patients would suffer from any discomfort, the elongated or calcified styloid process would be resected surgically.
The significance of this case was that styloid process calcification and elongation were manifested as the same pattern in twins, which might imply that there might be a genetic factor to the cause of the elongation and calcification of the styloid process. This report might provide a clue about the unknown pathogenesis of the pathology.
Case Report
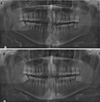
Two 30-year-old male patients visited the dental clinic for disabled at Seoul National University Dental Hospital. They were identical twins with mental retardation. They went through a routine dental check-up and radiographs were taken as aids to examine their oral health. On panoramic radiographs, both of the patients were presented with mesially impacted mandibular third molars, dental caries, and slight alveolar bone resorption. In addition, they both had bilateral calcified stylohyoid complex (Fig. 1).
Using the measurement method by Jung et al5 for calcified stylohyoid complex, the length of styloid process were measured. One patient showed the severely calcified stylohyoid ligament on the right side, measuring 84.4 mm in length and 11.2 mm in width. The left stylohyoid ligament was partially calcified measuring 55.2 mm in length and 5.17 mm in width. The other patient also showed the severely calcified stylohyoid ligament on the right side measuring 72.3 mm in length and 8.3 mm in width. The left stylohyoid ligament was partially calcified measuring 67.8 mm in length and 4.3 mm in width. The pattern of calcification was similar; both sides of the calcification involved the regions of tympanohyal, stylohyal, and ceretohyal, and the calcification on the right side was thicker. They did not display such symptoms as neck pain or headache, and they had no history of trauma.
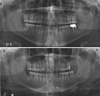
No surgical treatment was performed on both patients for the calcified stylohyoid complex. After dental treatment including extraction and caries treatment with root canal treatment, their follow-up images showed no changes of the calcified stylohyoid complex (Fig. 2).
Discussion
Elongated styloid process, a kind of soft tissue calcification, is commonly identified on panoramic radiographs. Since it usually does not impose any discomfort to patients, it is usually not treated surgically. Furthermore, it has been considered as a normal anatomic variant. However, some patients complain of neck pain, sore throat, foreign body sensation, and dysphagia, which require surgical interventions in addition to complete understanding of the etiology and the possibility of its relation to any syndromes.
The exact cause of the elongated styloid process due to calcified and ossified bone and ligament is unknown. It is believed that any trauma in the cervicopharyngeal region, especially after tonsillectomy, might stimulate a subsequent growth of the styloid process.7 There is a controversy over the relations between trauma history and calcified stylohyoid complex since there are many cases with no trauma history. In addition, it was suggested that local chronic irritations, surgical trauma, endocrine disorders in female at menopause, persistence of mesenchymal elements, growth of the osseous tissue, mechanical stress, or trauma during development of styloid process could result in calcified hyperplasia of the styloid process.
Even the twins had no history of trauma, they had stylohyoid complex calcification in the similar area in this case. Even though there were some reports on the relationship between calcified stylohyoid complex and numerous general medical conditions,6,7 there was no such literature which mentioned its genetic factor. Okabe et al8 found a significant correlation between the length of the calcified stylohyoid complex and serum calcium concentration level and heel bone density. Meanwhile, MacDonald-Jankowski9 reported the significant differences in morphologies of the stylohyoid complex between Londoners and Hong Kong Chinese. This racial difference might indirectly indicate the genetic effects on the calcification of stylohyoid complex.
However, there was no such report that suggested that stylohyoid complex calcification was caused by genome. This case suggests a possibility that the stylohyoid complex calcification might be originated from genetic factor.
 XML Download
XML Download