

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Since their conception in the 1900s, Rapid Palatal Expanders (RPE) have been widely used by orthodontists to treat maxillary transverse discrepancies.1-3 Previous studies on the skeletal effects of RPE therapy have been conducted using traditional two-dimensional radiographic analysis, dental casts, and acoustic rhinometry.4-7 More recently, cone-beam computed tomography (CBCT) imaging has been utilized to further study these skeletal effects to support, refute, or expand on the original findings.8-11
One of the biggest challenges with RPE appliances is the achievement of true orthopedic changes via skeletal expansion. A recent study has shown the overall results of RPE treatment produce 49% dental tipping, 38% skeletal expansion, and 13% alveolar tipping.9 Anatomical factors such as the large surface area of sutures surrounding the maxillary complex limit the sutural opening by creating more resistance to expansion superior and posteriorly.10 A CBCT study performed by Kartalian et al11 found an increased width of 2.08 mm, 2.25 mm, and 5.4 mm in the nasal floor, hard palate, and dental level, respectively.
It was reported that RPE therapy produces a significant increase in nasal width of 37.2% and a decrease in maxillary sinus width.9 Garib et al12 specified the increase in nasal floor width as equal to one-third of the expander's jack screw opening. More recently, Christie et al13 also reported a nasal width increase of 2.73 mm (33.23% of the jackscrew opening) at the first permanent molar.
One may assume a possible decrease in the dimensional characteristics of the maxillary sinuses due to the increase in nasal width. However, to date no study reported the volumetric changes in the maxillary sinuses in accordance with maxillary expansion. The aim of this study was to examine the dimensional changes of skeletal and dental structures in a group of growing patients treated for maxillary constriction before and after RPE treatment with Hyrax appliance using CBCT imaging with particular emphasis on the nasal cavity and concomitant maxillary sinus volume changes.
Materials and Methods
Approval for the study was granted by the Institutional Review Board of the University of the University of Texas Health Science at Houston. Patients diagnosed with bilateral posterior crossbites who were in need for bilateral maxillary expansion determined by an experienced orthodontist were examined. Excluded were the individuals that had craniofacial anomalies, compliance issues, the need for surgically assisted Rapid Maxillary Expansion RME, and previous orthodontic treatment history. Thirty patients (20 females, 10 males) were included in this study (mean age 13.8 years; range, 9 years to 20 years). Comparisons were made between pre- and post-treatment measurements. Additionally, treatment changes were compared between two different age groups (Group 1: 9-14 years (n=18; 12 females, 6 males), Group 2: 15-20 (n=12; 8 females, 4 males)) to determine whether there was any age related difference in the parameters studied. The intermaxillary suture becomes more tortuous and interdigitated with development14 thereby resisting the orthopedic expansion. Therefore, we aimed to compare actively growing individuals (Group 1) to individuals with decelerated/minimum growth potential (Group 2).
All patients were treated with a Hyrax appliance that was either 2-banded (supported by bilateral maxillary first molars with extension of expansion arms along the gingiva of the premolars) or 4-banded (supported by bilateral maxillary first premolars and first molars). The appliance was activated by two-turns a day until the maxillary alveolar arch constriction was overcorrected. Each patient took CBCT images available before and after maxillary expansion therapy. The expansion time was 3-4 weeks with a mean of 22.3 days.
The T1 images were taken prior to orthodontic treatment, and the T2 images were obtained immediately after the completion of maxillary expansion activation.
Galileos Comfort (Sirona Dental Systems GmbH, Bensheim, Germany) X-ray unit was used to capture the CBCT images of the individuals with exposure parameters of 85 kVp, 21 mA, 14 seconds, and 0.3 voxel size. The patients were positioned so that they faced outward during imaging. In addition, the forehead support and chin rest of the scanner were used to stabilize the patients' head with teeth in maximal intercuspation. Linear and angular measurements were made with Sidexis XG software (Sirona Dental Systems GmbH, Bensheim, Germany). Dolphin 3D software (Dolphin Imaging, Chatsworth, CA, USA) was used to obtain the data for volumetric analysis. All CBCT measurements were standardized at the level of the inspected anatomic landmarks perpendicular to midsagittal plane using reslicing function of the software.
Determining the amount of dental effects
Effects of expansion on teeth
Two-dimensional axial images were created perpendicular to the midsagittal plane in order to measure the amount of dental expansion. Coronal view was used to determine the location of cemento-enamel junction (CEJ) of each tooth. Measurements were taken at each of the two time points (T1 and T2) at the level of both maxillary premolars and canine. The measurement recorded the distance between the left and right maxillary second premolar at the most palatal aspect of the CEJ. The same measurements were taken for the maxillary first premolar and canine, respectively (Fig. 1A).
Palatal vault angle
Two-dimensional coronal sections were used to measure the palatal vault angle at each time period (T1 and T2). To measure the palatal vault angle, an angle was created between two lines extending from the most inferior aspect of the midline of the hard palate extending to the CEJ of the maxillary first molars, bilaterally. This measurement was made at a point coronally at the palatal root of the first molars (Fig. 1B).
Determining the amount of skeletal effects
Foramina to foramina measurements
Measurements of linear distances were recorded from the axial section of the T1 and T2 images at the level of each of the following: the width of the incisive canal (Fig. 2A) measured from lateral wall to lateral wall, the greater palatine foramen to contralateral greater palatine foramen (Fig. 2B), and the infraorbital foramen to contralateral infraorbital foramen (Fig. 2C).
Linear measurements of the position of the hard palate
Measurements of linear distances were recorded from the sagittal section of the T1 and T2 images to record each of the following: Sella to Nasion, Sella to Posterior Nasal Spine (PNS), Sella to Anterior Nasal Spine (ANS), Nasion to ANS, and Nasion to PNS. The four anatomical landmarks were selected for their reproducibility and stability to obtain accurate measurements. In addition, each landmark can be precisely located within a sagittal slice of the CBCT image.
Nasal cavity width measurements
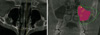
Measurements of linear distances were recorded from the axial section of the T1 and T2 images at the widest point of the anterior bony nasal cavity (Fig. 3A).
Maxillary sinus volume measurements
Maxillary left and right sinus volumes were individually measured at T1 and T2 using Dolphin 3D Sinus/Airway volume analysis software. To measure the individual volumes within the software, boundary lines were drawn surrounding the sinus cavity in the axial, coronal, and sagittal views individually. Seed points were then placed within the sinus cavities and boundaries until the entire sinus was included. The sinus volume was then generated by clicking the "Update Volume" tab. Left and right volume measurements were then added together to compare the two time points (Fig. 3B).
Statistical analysis
All of the recorded data from the two time periods (T1, pre-expansion, and T2, post-expansion) were compared and analyzed. Means and standard deviations were calculated for each parameter. To determine the accuracy of the measurements, the records of ten subjects were randomly selected from the original sample one month later and re-measured by the same operator. Intra-class correlation coefficients (ICCs) were used to determine the measurement reliability. Paired t-tests were performed for comparing pre- to post-expansion measurements. The two age groups were compared using Mann-Whitney U test. The significance level of p<0.05 was used for all statistical analyses.
Results
ICCs revealed a high level of agreement for all the variables (0.89≤single measure ICCs≤0.99). Effect size was calculated using the mean and SD of the T1-T2 differences for the total sinus volume measurement. A post hoc power test that is calculated with an effect size of 0.41 at the p=0.05 significance level, indicated 71% power for the study. The comparison of pre- to post-expansion images is presented in Table 1.
Dental effects
Effects of expansion on teeth
All the dental measurements showed increases as a consequence of Hyrax therapy. The mean dental expansion of the maxillary second premolar width from T1 to T2 was 3.34 mm (p<0.05). The mean dental expansion of the maxillary first premolar and maxillary canine widths from T1 to T2 were 2.96mm(p<0.05) and 1.62 mm (p<0.05), respectively.
Skeletal effects
Foramina to foramina measurements
To determine the amount of skeletal expansion, linear measurements were taken on reproducible landmarks, namely the bilateral incisive, greater palatine, and infraorbital foramen. Significant increases were found for the incisive foramen width (mean=0.87 mm, SD=0.97), the bilateral greater palatine foramina (mean=1.20 mm, SD=1.06), and the bilateral infraorbital foramina (mean=1.26 mm, SD=2.43).
Linear measurements of the position of the hard palate
None of the variables related to the evaluation of the position of the maxilla in the vertical and anteroposterior dimensions showed significant changes as evidenced by the pre- and post-expansion comparison of Sella to Nasion, Sella to PNS, Sella to ANS, Nasion to ANS, and Nasion to PNS.
Nasal cavity width measurements
The mean linear difference in the width of the anterior nasal cavity from T1 to T2 increased by 0.93 mm (p< 0.05).
Maxillary sinus volume measurements
Although individual variations existed in the study sample regarding the volumetric variables, before and after measurements proved that both the right and left side sinus volumes and a combined sum of them had negligible changes. The total volume difference of the left and right sinuses together differed only 69.33 mm3, on the average, between T1and T2 (P>0.05).
Discussion
Our results confirmed the fact that rapid maxillary expansion was effective at increasing the transverse dimension of the maxilla and the maxillary dentition. When evaluating the transversal plane changes, transversal width measurements consistently increased with dental expansion superseding the skeletal effects. Mean changes in the dental widths from T1 to T2 were 3.34 mm, 2.96 mm, and 1.62 mm at the second premolars, first premolars, and canines, respectively. Expansion at the level of the dentition was the greatest in the posterior and decreased anteriorly. This finding might be supported by the fact that the RPE was anchored to the first molars, and therefore dental tipping was expected in that region.
The palatal vault angulation increase found in this study showed how RPE therapy resulted in a combination of arch widening and reorganization of the hard palate. Recent studies13,15 have already shown how the palatal vault was reshaped and the palatal volume was increased upon the completion of expansion therapy.
To accurately measure the amount of skeletal expansion from RPE therapy, reproducible skeletal landmarks were required. Therefore, the greater palatine, infraorbital, and incisive foramina were used in this study. All of the measurements related to skeletal expansion were significant, as expected considering the age group of the study sample. Furthermore, judging by the ratio of the overall changes, the most to least expansion was observed at the incisive, greater palatine, and infraorbital foramen, respectively. These findings supported the pyramidal widening of the maxilla with RPE treatment. This phenomenon was due to the decreased resistance to expansion from the maxillary complex and associated structures as moved anteriorly and inferiorly; and the fact that the RPE was a tooth-borne appliance, which elicited more of a dental than skeletal response.6 In addition, anatomical factors such as the large surface area of sutures surrounding the maxillary complex influenced this outcome by creating more resistance to expansion.10,11,16
The variables related to the anteroposterior and vertical position of the maxilla, yielded no significant changes between pre- and post-expansion. Therefore, our findings did not support the view17 that anterior and inferior migration of the maxilla occurred as a consequence of rapid maxillary expansion therapy. In a CBCT evaluation study15 of the maxillary palatal vault AP, as a dimensional characteristic, length was also reported as virtually stable in patients with rapid palatal expansion. These findings might suggest that almost no anteroposterior change related to maxillary expansion therapy should be expected, if not minimum.
Our results indicated a significant increase in the nasal cavity width as a result of RPE therapy, but to a lesser extent than previously published papers.11,13 The difference between previous reports and our study could be explained by the variations in the measurement techniques since we performed our measurements at a relatively more anterior location. However, according to our results no significant change was observed in the volume of the maxillary sinuses due to expansion therapy. It has been recently claimed that RPE treatment caused a widening of the nasal cavity and a concomitant narrowing of the maxillary sinus widths.9 Assuming the statement by Garrett et al9 was correct, the maxillary sinuses might be undergoing a reshaping process. Accordingly, expansion therapy might actually not affect the volumetric size.
At this time, further research is encouraged to aid the clinician's knowledge of the secondary effects caused by rapid maxillary expansion. It is apparent that we might not fully interpret the relationship between successful expansion treatment with dental and skeletal changes and associated adaptations. As three-dimensional CBCT technology and software programs improve, further studies using the CBCT technique will ultimately define the limits of these scans.
In short, within the limitations of this study, nasal cavity width increased with Hyrax expansion therapy. However, no associated change in maxillary sinus volumes was observed.



 XML Download
XML Download