

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Odontomas are classified as odontogenic tumors; however, due to their limited and slow growth, they are considered to be hamartomas in which all dental tissues are represented, rather than benign neoplasm.1-3 On the basis of gross, radiographic, and microscopic features, odontomas are sub-classified into compound odontoma (small toothlike structures) and complex odontoma (a conglomeration of dentin, enamel, and cementum).1-5 Similar to teeth, once fully calcified, they do not develop further, and multiple odontomas are rare.6 In general, they constitute 22% of all odontogenic tumors of the jaws.7 The etiology of odontoma is unknown, but genetic factors, family history, and environmental causes such as trauma and infection have been suggested.1,5,6,8 The radiographic findings of odontomas depend on their stage of development and degree of mineralization. The first stage is characterized by radiolucency due to lack of calcification. Partial calcification is observed in the intermediate stage, while in the third stage the lesion usually appears as radiopaque masses surrounded by radiolucent areas corresponding to the connective tissue histologically.2,5 Odontomas are generally asymptomatic, often associated with delayed eruption, or impaction of permanent teeth.1-3,6,7,9-11 There have been many studies of odontomas dealing with clinical investigations, radiographic features,1,2,12-15 and case reports,5,7,8,16,17 however, these investigations included no results of treatments associated with the impacted permanent teeth according to age. The aim of the present study was to evaluate the clinical findings and results of treatment of odontomas focused on the associated impacted permanent teeth.
Materials and Methods
We investigated 73 odontomas in 72 patients who visited Kyungpook National University Dental Hospital from April 2004 through November 2011. Their medical records, features on the panoramic radiographs, and pathological reports were investigated.
The panoramic radiographs had been acquired by OP-100 (Instrumentarium Imaging Co., Tuusula, Finland). The diagnoses had been confirmed by radiographic or histopathologic examination and all complex odontomas had been confirmed by histological examination.
The patients' data gathered in this study included their age, gender, location, chief complaints at presentation, effects on dentition, and treatment of the odontoma and associated impacted tooth. Also, two oral and maxillofacial radiologists interpreted the panoramic images using INFINITT PACS software (Infinitt Co., Seoul, Korea) on a 3 megapixel diagnostic gray display system, ME311L (Totoku Electric Co., Tokyo, Japan).
The Fisher's exact test was used to assess the relationship between the patients' ages at the initial detection and the preservation of the impacted permanent tooth. Statistical analysis was performed by using IBM SPSS statistics 19.0 for Windows (SPSS Inc., Chicago, IL, USA) and p<0.01 was considered to indicate statistical significance.
Results
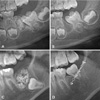
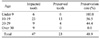
The distribution of 73 odontoma patients' age and gender are presented in Table 1. There were 45 cases of compound odontomas and 28 cases of complex odontomas in this study. In the cases of complex odontomas, two complex odontomas were found in a patient on both sides of the maxillary posterior area. Most compound odontomas were found in the second decade of life, while complex odontomas were not related to the age distribution. Odontomas showed no gender predilection and compound odontomas were one and a half times more common than complex odontomas. Fifty-five cases (75.3%) of 73 odontomas were detected on routine dental examinations (Table 2). Twenty-seven of 45 compound odontomas (60.0%) occurred in the canine area. In contrast, 16 of 28 complex odontomas (57.1%) were found in the molar areas (Fig. 1). Impaction of permanent teeth (61.6%) was the most common effect on the adjacent teeth, followed by prolonged retention of deciduous teeth (32.9%), and displacement of the adjacent teeth (30.1%) (Table 3). Most odontomas (84.9%) were removed surgically, and the impacted permanent teeth associated with the odontomas were managed by surgical removal (53.2%), orthodontic treatment (25.5%), or surgical repositioning (6.4%) (Tables 4 and 5). Forty-five of 73 odontomas (61.6%) caused 49 impacted permanent teeth and a maximum of 3 teeth were impacted per odontoma. Since one patient refused treatment, 47 impacted teeth were treated in 44 patients. Twenty-three teeth were saved through orthodontic treatment, surgical repositioning, and normal eruption, while 24 teeth were removed (Table 6 and Fig. 2). All impacted teeth were preserved in those under 9 years old, while all were removed over 30 years old. In the patients between 10 and 29 years of age, the treatment methods were affected by the position of the impacted teeth. There was a statistically significant relation between their age and the preservation of the impacted permanent tooth associated with odontoma (p<0.01).
Discussion
There have been many reports of odontomas, however there were relatively few studies that reported more than 100 cases of odontomas.1,12-15 According their studies, the male incidence was 48-52.9% suggesting no gender predilection. In the present study, the male incidence was 47.9% (35/73). Odontomas develop and mature while the corresponding teeth are forming and cease development when the associated teeth complete development.3,6 Many studies reported that odontomas were usually detected in the second decade of life.1,12-15 In the present study, 34.4% of them were also found in the second decade, followed by 21.9% in the third decade, and the youngest patient was 5 years old.
As for location, the incidence of odontomas in the maxilla was 50.9-66.7%.1,2,12-15 The most common location was the anterior region of maxilla2,12,15 and the incisor lesion was diagnosed and treated earlier than the canine or third molar lesions.14 In the present study, the most common locations were, respectively, the canine region for the compound odontoma and the molar region for the complex odontoma, which corresponded with the reports of Kulkarni et al7 and da Costa et al.16 Odontomas rarely involved the primary dentition (1.3-12.8%)2,15 and in the current study, none of the odontoma involved the primary dentition.
Many studies have reported various disturbances to tooth eruption related to odontomas.2,5-7,9,14,16,18,19 Katz14 studied 396 cases of odontomas in all age groups and found that 41% were associated with unerupted teeth. Tomizawa et al2 and Kaugars et al15 reported that 47.6% (167/351) and 87% (34/39) of odontomas caused tooth impaction, respectively. In the present study, 63% (46/73) of odontomas resulted in eruption disturbance. Although more than half of them caused eruption disturbance, 75.3% of them were detected on routine radiographic examination. This result was different from that of the previous study2 in which delayed tooth eruption was the most common chief complaint of odontomas. This might be originated from the current situation that panoramic radiographs have been widely used for routine examination. Only 9.6% of odontomas were presented with delayed eruption in comparison with a high incidence of eruption disturbance.
Surgical removal with or without denudation of the impacted teeth has been usually performed for treatment of odontoma.2,6,17 There has been no general agreement on the best management approach for impacted teeth associated with odontomas. The treatment options comprise surgical extraction, and surgical opening and postsurgical clinical and radiological controls to evaluate the course of these teeth.3,7,9,17 Morning18 examined 42 cases of impacted teeth related to odontomas and reported that removal of the odontomas in the primary operation led to the eruption of the impacted teeth in 45% of cases, with a second surgical and/or orthodontic intervention giving better results. Eight of 25 impacted teeth erupted spontaneously after surgical removal of odontomas in the study of Tomizawa et al.2 In their study, the patients had been observed more than 3 months after the first removal and then if the impacted teeth had not erupted, surgical exposure of the tooth crown with or without orthodontic traction had been performed. In the present study, 23 of 47 impacted teeth (48.9%) were preserved through various treatments such as surgical removal, orthodontic treatment, observations for normal eruption, and surgical repositioning.
The early diagnosis of odontomas allows the adoption of less complicated and expensive treatment, and ensures better prognosis.19,20 In this study, all of the impacted teeth were saved in those under 9 years old, while all of them were removed in those over 30 years old. The preservation rates were 56.5% and 44.4% in the patients in the second and third decade of life, respectively. The average age for spontaneous eruption was 7.7 years old. These findings were in close agreement with the results of de Oliveira et al.20 Kodali et al5 emphasized the importance of routine examination using panoramic radiography for early detection of odontomas and prevention of adverse effects.
The panoramic examination as a supplement to clinical examination in the national oral examination performed in Korea might improve the public oral health.21,22 The radiation doses from two panoramic radiographic equipments with a charge-coupled device (CCD) sensor were 14.2 or 24.3 µSv. These doses were same as 1.7 and 3.0 days additional background radiation.23 Although more studies would be required to develop selection criteria for panoramic radiography as a national oral examination tool,22 it would be beneficial to take a panoramic radiograph in the first decade for the early detection of odontomas and prevention of impacted permanent teeth. Considering tooth development and incidence of odontomas, another radiographic examination would be also recommended during the second decade of life.
In conclusion, most odontomas were found in the second decade of life on routine radiographic examination and they could cause impaction of the adjacent permanent teeth. Early detection and treatment of odontomas could increase the possibility of preservation of the impacted teeth through various treatments. Therefore, periodic panoramic examination in the first and second decades of life would be recommended for the early detection and better prognosis of odontomas.






 XML Download
XML Download