

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Supernumerary teeth or hyperdontia are defined as the existence of an excessive number of teeth in relation to the normal dental formula,1 and they may develop at any location in either upper or lower dental arch. While single tooth impaction is not uncommon, development of multiple impacted teeth is a rare condition and often found in association with syndromes or developmental anomalies such as cleidocranial dysplasia, Gardner's syndrome, trichorhino phalangic syndrome, and cleft lip and palate. However, it can be present in patients without any systemic pathology. The presence of supernumerary teeth can cause alterations in neighbouring teeth, commonly retained teeth or delayed eruption, ectopic eruption, dental malposition, occlusal problems, diastema, and rotation.2
Supernumerary teeth which are well aligned in the arch and resemble the normal anatomy of adjacent teeth are called supplementary teeth. There are evidences of occurrence of supplementary premolars and molars (fourth molar/distomolar/paramolar)3 in the pre-historic man. According to Darwin's theory of evolution, as human evolved, the organs of minimally used became vestigial, which were appendix, tail bone, fourth molar. However, in rare cases there are still occurrence of supplementary molars and supplementary premolars.
The precise aetiology of supernumerary teeth is unknown, however several theories have been postulated to explain their presence: an abnormal reaction to a local traumatic episode, environmental factors, the phylogenetic theory as a regression to the anthropoids whose dental formula had more teeth, dichotomy of the tooth germ and the theory of hyperactivity of the dental lamina, the autonomic recessive inheritance or linked to the X chromosome, are accepted broadly.4-6
This report presents five cases of the patients who had supernumerary teeth without any associated syndrome or development anomaly.
Case Report
Case 1
A 42-year-old male patient visited the Oral Medicine and Radiology unit of NHDC, Mumbai in 2009. He was referred by his family dentist, complaining pain in the left mandibular angle region. He had difficulty in chewing on the left side and the mouth opening was normal. On the examination, the gingival operculum distal to the third molar was inflamed and tender on palpation. The left mandibular third molar appeared completely erupted and well aligned, however a tooth-like structure with black discoloration appeared to be embedded distal to the third molar (Fig. 1A). The provisional diagnosis was pericoronitis and a lateral oblique radiograph was advised in order to evaluate the region accurately. There was no relevant familial history of dental abnormalities. The patient did not show any structure beyond the third molars in three other quadrants. The lateral oblique radiograph for the left mandible revealed the presence of a partially impacted supernumerary tooth distal to the third molar. The shape of the supernumerary tooth was similar with a molar but smaller in size, single rooted and distally inclined, thus it could be defined as a supplementary distomolar. The radiograph showed a large periapical lesion associated with the supplementary tooth (Fig. 1B). We decided to extract the fourth molar since the patient had discomfort due to pericoronitis and irreversible pulpitis.
Case 2
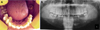
A 36-year-old male patient visited our department with a complaint of missing tooth in the lower left premolar area. The patient was in a normal health condition generally. On the clinical examination, it was noted that besides the missing tooth, the patient also had a supernumerary tooth distal to the right maxillary third molar which was placed palatal and distal to the third molar. There was no presence of any other supernumerary teeth in the other quadrants. There was no any other specific oral finding (Fig. 2A) and relevant familial history of dental abnormalities.
Panoramic radiograph revealed only one supernumerary tooth distal to the right maxillary third molar. The roots of the third molar and the supernumerary tooth were overlapped and difficult to visualize them independently, however the morphology of the crown resembled a mini-sized molar, hence it was diagnosed as a supplementary distomolar (Fig. 2B). As there was no complaint and the fourth molar was not clinically impeding the patient's day to day activity, it was decided not to give any further treatment.
Case 3
A 36-year-old male patient visited our department with a complaint of replacement of missing teeth. The patient was otherwise in a normal health condition. On clinical examination, the right maxillary first molar was absent. In addition, a supernumerary premolar-like tooth, distal to the right maxillary second premolar was observed, as well as a second premolar in the left maxilla was missing. The upper third molars in both sides were erupted and well aligned in the arch, while the mandibular third molars in both sides were not found clinically. In the lower right quadrant, a total of four, well-aligned, premolar-like teeth were observed. The tooth distal to the canine appeared as the first premolar, the tooth distal to that appeared as a mini-sized second premolar, and the following two teeth had the same anatomy and size with the second premolar. Thus, it was difficult to distinguish them as rather permanent or supplementary. In the lower left quadrant, the first premolar had caries and the second premolar was retained root state, followed by two more teeth (Fig. 3A). Due to the destruction of the crown, it was difficult to distinguish which was the permanent or the supplementary tooth. There was no relevant familial history of dental abnormalities. Panoramic radiograph confirmed these clinical findings and additionally revealed an impacted supernumerary tooth mesial to the first molar in the left mandible (Fig. 3B). There was no impacted lower third molar in the mandible.
It was decided not to extract the erupted supernumerary teeth since the patient had no complaint and the occlusion was not impeded. However, before giving prosthesis in the upper right first molar region, alignment of the supernumerary had to be considered. The patient was referred for endodontic treatment of the caries lesion of the lower right premolar and to an oral surgeon for extraction of the retained root. Also, the opinion on the impacted supernumerary tooth was requested if it could affect the lower left first molar or the impacted supernumeraries would develop into cystic lesions.
Case 4
A 35-year-old male patient visited our department with a chief complaint of mild pain and food impaction in the upper right posterior region. On the examination, the upper right first molar had caries. On further intraoral examination, it was found that the patient had three supernumerary teeth lingual and distal to the second premolar in the lower right quadrant (Fig. 4A). Since the patient had pain on the upper right first molar, the endodontist suggested that the patient needed to extract the supplementary teeth in the lower right mandible to prevent food impaction on that area.
The patient was referred to an oral surgeon to extract them and panoramic radiograph was taken. The radiograph showed an impacted supernumerary tooth on the left lower mandibular area, which was placed apical to the lower left second premolar (Fig. 4B). An intraoral radiograph of the same region also showed the presence of a dilacerated premolar-like tooth; its root was placed apical to the mesial root of the mandibular first molar, and the crown was in the apical and buccal aspect of the left mandibular second premolar. The shape of the crown showed aberration in shape (Fig. 4C).
Case 5
A 20-year-old male patient visited our department for routine dental check up, prophylaxis, and replacement of the missing left lower molars which had been extracted. On intraoral examination, the left mandibular first and second molars were missing and a rotated supplementary premolar-like tooth, distal to the second premolar, was observed. On the right side of the mandible, the first molar was missing and there were two supplementary premolar-like teeth which were rotated and placed lingual to the premolars (Fig. 5A). Panoramic radiograph confirmed these clinical findings, and additionally revealed an impacted supernumerary tooth below the left mandibular premolars, with the crown facing towards the midline. The apex of the impacted supernumerary tooth was below and distal to the supplementary tooth (Fig. 5B).
The patient was referred to a prosthodontist to get an opinion if the presence supernumeraries in the lower right region might impede the placement of prosthesis. The patient was also informed not to extract the impacted supernumerary tooth as it was asymptomatic.
Discussion
Multiple supernumerary teeth not associated with syndromes are rare conditions. Yusof in 19907 reported that the premolar region in the lower arch was the most common area having supernumerary teeth. In our cases, three cases showed the presence of the multiple supernumerary teeth in the premolar area of all the quadrants and two cases showed an extra molar distal to the third molar.
The occurrence of non-syndromic supernumerary teeth is more often in maxilla than in mandible,8 in male than in female,9 in permanent dentition than in primary dentition, and unilaterally than bilaterally.10 Patients with non-syndromic supernumerary teeth might be related to heredity factor, therefore familial history should be carefully examined.
Maintaining a supernumerary tooth could result in the appearance of different abnormalities. Hegde and Munshi11 and Mason et al12 reported the displacement, rotation, ectopic eruption, and malocclusion of adjacent teeth due to supernumerary teeth in their studies, and similar alterations were noted in our cases, related to the position and orientation of the supernumerary teeth.
The clinical and radiographic examinations are important for a substantial treatment plan which varies from simple extractions to orthodontic/prosthetic treatment for obtaining correct occlusion. However, it is difficult to establish an ideal treatment for those of multiple supernumeraries cases.
All the cases reported were found in male patients. Four cases showed the supernumeraries in the mandible and one in the maxilla. Three cases showed the presence supernumeraries in the premolar region bilaterally. Patient with non-syndromic supernumerary teeth need to have periodical radiographic observation if he/she is asymptomatic. Then, it is advisable to remove these supernumerary teeth immediately if it starts to show any pathologic change.
In all the five reported cases except for Case 1, the patients had no discomfort associated with the supernumerary teeth. However, we still emphasize the importance of a precise clinical history and radiographic examination when patients with multiple supernumerary teeth visit for consultation since most of them are associated with other dental anomalies and syndromes. Then the related clinical problems should be considered primarily than treating the presence of the supernumerary teeth.




 XML Download
XML Download