

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dentigerous cysts are the most common developmental, odontogenic cysts arising from a crown of impacted, embedded, or unerupted teeth. The exact pathogenesis of these cysts is unknown. They are believed to originate from the follicle of the unerupted tooth. These cysts are caused by expansion of dental follicles resulting from accumulation of fluid between the tooth crown and epithelial components.1 Dentigerous cysts are the second most common odontogenic cysts after radicular cysts, accounting for approximately 24% of all true cysts in the jaws.2 Dentigerous cysts around supernumerary teeth account for 5% of all dentigerous cysts, most developing around a mesiodens in the anterior maxilla.3 A mesiodens, a kind of supernumerary tooth, is located in the maxillary central incisor region. A mesiodens has an overall prevalence of 0.15-1.9%. A mesiodens can occur individually or in multiples and often does not erupt. Mesiodens sometimes bring about median diastema, delayed eruption of the permanent central incisors, alteration of the position of the permanent incisors, and dentigerous cyst formation.4 This report described two cases of a rare entity of dentigerous cyst associated with an impacted mesiodens.
Case Report
Case 1
A 55-year-old male patient reported to the Department of Oral Medicine, Diagnosis, and Radiology with a chief complaint of pain and swelling in the maxillary anterior region for 1 month. Since then, the swelling had gradually increased in size. The patient had taken an unknown medication for the pain and swelling, but he had no relief. On clinical examination, a solitary diffuse extraoral swelling was seen in the upper anterior region of the face. It had anteroposteriorly extended from the tip of the nose to 1 cm lateral to the left ala of the nose, superoinferiorly extending from 2 cm inferior to the left inner canthus of the eye to the inferior border of the upper lip. The tip of the nose was slightly deviated towards the right, and the left nasolabial fold was elevated (Fig. 1A). On intraoral examination, a solitary well-defined intraoral swelling measuring about 3 cm×3 cm was seen in the maxillary anterior labial vestibule extending from the left central incisor up to the left first premolar. The swelling was roughly oval in shape. The swelling was tender on palpation and fluctuant in consistency. The overlying mucosa was bluish in color, and the superficial blood vessels were prominent (Fig. 1B). The left lateral incisor, canine, and first premolar showed grade III mobility and were tender on vertical percussion.
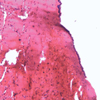
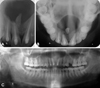
On radiographic examination, the maxillary topographic occlusal radiograph showed a well-defined, round, corticated radiolucency in the anterior maxillary region. A dilacerated supernumerary tooth was seen lying horizontally with the crown facing towards the center and root near the anterior border of the lesion (Fig. 2A). The panoramic radiograph showed a well-circumscribed, corticated radiolucent lesion in the anterior maxilla, crossing the midline and extending from the right maxillary first premolar to the left maxillary first premolar. Slight root resorption was seen in association with the right central and lateral incisors, and severe root resorption was seen in association with the left lateral incisor and canine (Fig. 2B). On a computed tomography (CT) scan, the coronal section showed a large, radiolucent, well-defined lesion in the anterior maxilla with a supernumerary tooth seen towards the inferior border of the lesion. There was upward displacement of the floor of the nasal cavity and of the floor of the maxillary sinus of the left side. The axial section showed complete destruction of the anterior border of the lesion (Fig. 2C). A provisional diagnosis of the infected cyst was made on the basis of the patient's history, clinical examination, and radiographic examination. On aspiration, a viscous brick-red colored fluid was suggestive of an infectious cyst. The lesion was surgically enucleated along with removal of the impacted mesiodens, and the maxillary anterior teeth were extracted (Fig. 3). The histopathological examination showed a cystic lumen with a very thin lining of stratified squamous epithelium and dense fibrocellular connective tissue stroma with chronic inflammatory infiltrate, suggestive of an infected dentigerous cyst (Fig. 4). The patient remained asymptomatic, and no complications were noted after 1 year follow-up.
Case 2
A 46-year-old male visited our department with chief complaints of pain and swelling in the maxillary anterior region of the jaw for the past 3 years. Prior to visiting our department, the patient had visited a dental institute and had undergone endodontic treatment of his maxillary anterior teeth. The swelling had regressed slightly after the treatment; however, the swelling started increasing gradually in size and had reached the present size. The swelling was also accompanied by dull, throbbing pain from 1 month prior to the visit. On clinical examination, solitary diffused extraoral swelling was seen in the upper anterior region of the face. It was anteroposteriorly extending from the tip of the nose to 1 cm lateral to the left ala of the nose and superoinferiorly extending from the ala-tragus line to the inferior border of the upper lip. The tip of the nose was slightly deviated towards the right along with elevation of the left nasolabial fold (Fig. 5A).
On intraoral examination, solitary well-defined intraoral swelling measuring about 3.5 cm×3 cm was seen in the maxillary anterior labial vestibule extending from the maxillary right lateral incisor to the maxillary left canine. The swelling was roughly oval in shape. The swelling was tender on palpation and fluctuant in consistency (Fig. 5B). The maxillary right and left central incisors and the right lateral incisor showed the presence of a temporary restoration. The maxillary central and lateral incisors were tender on percussion (Fig. 5B).
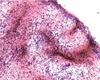
On radiographic examination, an intraoral periapical radiograph showed the presence of large, well-defined, corticated periapical radiolucency along with an impacted mesiodens. Root resorption was seen with the right central incisor. A radiopaque filling material was seen in the root canals of the right and left central incisors and the right lateral incisors (Fig. 6A). Maxillary topographic occlusal radiograph showed a well-defined, round, corticated radiolucency in the anterior maxillary region. The radiolucency was not associated with the apices of the teeth. A dilacerated supernumerary tooth was seen lying horizontally in the radiolucent lesion (Fig. 6B). Panoramic radiograph showed a well-circumscribed, corticated, oval, radiolucent lesion in the anterior maxilla, extending from the mesial root surface of the right first premolar to the distal root surface of the left canine (Fig. 6C). A provisional diagnosis of the infected dentigerous cyst was made on the basis of the patient's history, clinical examination, and radiographic examination. The lesion was surgically enucleated along with the removal of the impacted mesiodens. Histopathologic examination confirmed the diagnosis of an infected dentigerous cyst (Fig. 7).
Discussion
After the radicular cyst, the dentigerous cyst is the second most common type of odontogenic cyst and is always associated with the crown of an impacted, embedded, or otherwise unerupted tooth. Dentigerous cysts are typically asymptomatic and may be large, destructive, expansile lesions of a bone. The highest incidence of dentigerous cysts occurs during the second and third decades.5 However, in our cases it was diagnosed at a much later age. The cyst usually occurs in the mandible, and is known to be both unilocular and multilocular and causes apical resorption of the adjacent teeth, as observed in our patient. The diagnostic feature of this cyst is the presence of the unerupted tooth in its cavity, which in our cases was a mesiodens.6
A mesiodens is known to have a cone-shaped crown and a short root, as seen in our patients. It is a rare entity with a reported incidence of 0.15% to 1.9%, and it has a slight predominance in males.6 Dentigerous cyst formation is another problem that may be associated with supernumerary teeth. Primosch reported an enlarged follicular sac in 30% of the cases, but the histological evidence of cyst formation was found in only 4-9% of the cases.7 According to Asaumi et al,4 dentigerous cyst formation arising from the supernumerary teeth comprises 11% of cases. A further study found that 6% of supernumerary teeth have dentigerous cyst development, and Hurlen and Humerfelt suggested that dentigerous cysts associated with the supernumerary teeth occur in 7% of cases.8
Radiographically, the dentigerous cyst typically appears as a well-circumscribed, unilocular, usually symmetric radiolucency around the crown of an impacted tooth. An important diagnostic point is that this cyst attaches at the cementoenamel junction. The internal aspect of the cyst is completely radiolucent except for the crown of the involved tooth. One of the most difficult conditions to distinguish in the differential diagnosis is hyperplastic follicle. Other conditions that must be excluded in the diagnosis are odontogenic keratocyst, ameloblastic fibroma, and cystic ameloblastoma.3,9,10 Water's, panoramic, and skull radiography are simple and inexpensive methods that can be used in daily practice. The structure of a tooth can be clearly detected on panoramic radiographs. Therefore, panoramic radiographs are preferred over CT.1 Although the structure of a tooth can be clearly detected on panoramic radiographs, they are inadequate for localizing maxillary ectopic teeth due to their inherently less sharp image and ghost image. CT scan provides superior bony detail, allowing for the visualization of the size and extent of the lesion with determination of orbital or nasal invasion or involvement.11 Therefore, CT may be more valuable than plain film radiographs, not only for definitive diagnosis, but also for evaluation of the associated pathology, exact localization of the ectopic tooth, and proper treatment planning.12
The standard treatment for a dentigerous cyst is enucleation and extraction of the cyst-associated impacted or unerupted tooth. However, large lesions can be marsupialised. Histologically, dentigerous cysts are lined by a layer of nonkeratinized stratified squamous epithelium, with a surrounding wall of thin connective tissue containing odontogenic epithelial rests.1
In summary, although a dentigerous cyst associated with impacted permanent teeth is not uncommon, such development as a result of an impacted supernumerary tooth might be rare. Therefore, supernumerary teeth should be examined carefully to prevent harmful effects on the adjacent regular teeth and possible cystic development.




 XML Download
XML Download