

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The use of digital radiography in dentistry is increasing, and it is an alternative to film-based images. Because radiographic images can be manipulated using inversion, brightness and contrast control, zooming, and embossed tools, digital radiography also offers the possibility in radiographic interpretation of improving the detection of lesions as periodontal bone loss.1-4
There have been studies that have evaluated periodontal bone loss using digital images and film-based radiographs, and there has been agreement among the results.5-8 However, two studies have found differences between direct digital images and film-based radiographs in relationship to bone-defect measurements, and the results have shown the superiority of the digital images over the film-based radiographs.5,6
Of the types of manipulations performed on digital radiographic images, the most commonly used are brightness and contrast adjustments,9 and the examiners can adjust the images according to their preferences using dedicated and non-dedicated programs.2 Moreover, inverted digital images have been used for different dentistry procedures such as periodontal bone loss measurements3 and detection of the mandibular canal and mental foramen.2 However, there has been a lack of studies that deal with periodontal bone defects measurements using inverted digital images and software for general applications such as Adobe Photoshop.
The aim of this study was to compare periodontal bone defect depth measurement by inverted digital images and film-based images in dry pig mandibles.
Materials and Methods
Forty 2-wall bone defects were created in 40 hemi-mandibles from domestic pigs (Sus scrofa) using slow-speed #4 round diamond burs (KG Sorensen, Agerskov, Denmark). The depth of the bone defect was randomly determined, and the bone defect width was created based on the diameter size of the bur. The defect was created on the mesial side of the first premolar in the apical direction. Part of the mesial wall and the buccal wall were removed; the lingual and distal walls were left intact. A chisel was used to refine the borders of the defects. A tiny mark was made at the cementoenamel junction with a double-faced diamond disk to establish the upper border of the bone defect, and it was used as a reference point when taking the measurements.4
Image acquisition
Two periapical radiographs were taken of each defect using a direct digital system (CMOS Schick sensor, Schick Technologies Inc., Long Island, NY, USA) and F-speed film (Insight, Eastman-Kodak Co., Rochester, NY, USA). The characteristics of the original digital images were as follows: 40 µm pixel size, 900×641 pixels, 8 bits, and saved in tagged image file format (TIFF). There were a total of 80 images: 40 inverted direct digital images and 40 film-based images.
The radiographs were taken with the vertical long axis of the hemi-mandible fixed perpendicularly to the central ray and parallel to the sensor and film at a 40-cm focal spot-to-object distance. The geometric alignment between the sensor or film and the hemi-mandible was standardized using a fixing device. The dental X-ray unit (GE1000, General Electric Company, Wisconsin, USA) operated at 70 kVp and 10 mA. The exposure time for the digital images was 12 impulses and for the F-speed films it was 15 impulses. A 2-cm-thick wooden block was placed in front of the mandible in order to simulate the soft tissue.2 The film-based radiographs were processed with a Dentix 9000 (Dentix, Elmsford, NY, USA). The digital images were saved and stored as TIFF files without compression (8 bits, with a resolution of 600 dpi, and a file size of about 700 KB) using computer software (CDR DICOM for Windows v. 3.5, Schick Technologies Inc., Long Island, NY, USA), and then the images were transferred to an image processing software (Adobe Photoshop 7.0, Adobe System Incorporated, San Jose, CA, USA). The Adobe Photoshop software was used to create the inverted digital images. The levels of brightness and contrast were adjusted according to the examiners' individual preferences.10
Bone-defect measurement
The depth measurements of the defects were performed by four examiners as previously described:4 one experienced radiologist, two graduate students, and one undergraduate student on two types of images as well as on the dry mandibles. Inter-examiner agreement was obtained using consensus during the measurements of the defects, which were carried out in three consecutive sessions.
The digital inverted images were displayed on a 17-inch extended graphics array (WXGA) color monitor with a resolution of 1440×900 lines from a laptop computer (Satellite P-25-S507, Toshiba, Taiwan). The bone-defect depth was measured as the distance in millimeters from the deepest part of the defect to the cementoenamel junction; a tiny mark was used to facilitate the detection of the upper border of the bone defect using the ruler tool in Adobe Photoshop 7.0. Before measuring the defect depths in the digital images, all of the images were standardized according to a known length from the step wedge and the ruler tool in Adobe Photoshop 7.0 (Figs. 1A and B).
The digital and film-based images were interpreted under subdued lighting. A standard light box was used when reading the radiographs, and all extraneous light from the light box was blocked using black cardboard. The measurements in the film-based images were made using a digital caliper (Ultra-Call Mark III, Fowler, Geneva, Switzerland) from the reference point in the cementoenamel junction to the base of the defect. Direct visual measurements of all of the vertical osseous defects in the dry pig mandibles were made using a periodontal probe (Williams Probe, Hu-Friedy, Chicago, IL, USA), as described in a previous paper.2,4 This measurement was considered the standard depth (Fig. 2).
Statistical analysis
Student t test was used to compare the depth measurements obtained from the three methods, using the direct visual measurement as the standard for comparison with the other two as follows: the inverted digital images and direct visual measurement in the dry mandibles and film-based images and direct visual measurement in the dry mandibles. A significance level of 0.05 for a 95% confidence interval was used for each comparison.
Results
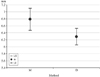
The results of the linear measurements of the two-wall bone defects using inverted digital images, film-based images, and direct visual measurements in the dry pig mandibles are shown in Figures 3 and 4.
There was a significant difference between the inverted digital images and direct visual measurements (p>|t|=0.0039). The means of the depth measurements on the inverted digital images and direct visual measurements were 6.29 mm (IC95%:6.04-6.54) and 6.79 mm (IC95%:6.45-7.11), respectively (Fig. 3).
There was no significant difference between the film-based images and direct visual measurements (p>|t|=0.4950). The means of the depth measurements on the film-based images and direct visual measurements were 6.64mm(IC95%:6.40-6.89) and 6.79mm(IC95%:6.45-7.11), respectively (Fig. 4).
Discussion
There was a significant difference between the measurements of the periodontal defect depth based on the two modalities of the images: the film-based image and inverted digital image. The results showed that there was a significant difference between the inverted digital image and direct visual measurements in the dry pig mandibles. However, the measurements on the film-based radiographs showed no statistical difference when compared with the direct visual measurements. Moreover, the linear measurements of the periodontal bone defects using an inverted digital image underestimated the amount of bone loss. Therefore, inverted digital images were found to be inferior to film-based images in the detection of periodontal bone loss.
Our results were in agreement with a previous study, in which the authors had performed embossed image manipulation.4 Although image manipulation in their study was different from that in our study, this agreement could be explained based on the fact that the radiographic interpretation tasks were the same, such as performing linear measurements using the same software (Adobe Photoshop) by the trained examiners. However, Tihanyi et al's study3 using inverted and unprocessed digitized images for periodontal bone loss measurements showed inconsistent results compared with ours. These inconsistent results could be explained by the adopted methodology such as the use of digitized radiographic images, and mainly because in the Tihanyi study there was no method used as standard for comparison with the imaging methods, such as the direct visual measurements in the dry mandibles that we used.
The most common digital image manipulations are contrast and brightness adjustments of the monitor11 during radiographic interpretation, creating a better image quality for the examiners based on their individual preferences.10 Some previously studies4,6,12-14 have compared manipulated and non-manipulated images in relationship to periodontal measurements and have not found any improvement in the diagnostic accuracy between these two types of image. Our study had the same results, in that the digital inverted images, such as the fact that the manipulated images, did not have better results than the film-based images.
The use of Adobe Photoshop for periodontal bone-defect depth measurements on the digital radiographic images was based on a previously published study,2 using four software systems: Schick dedicated software and non-dedicated software systems including VixWin 2000, Adobe Photoshop 7.0, and Image Tool 3.0. The results of that study showed that there was no significant difference in the detection of periodontal bone-defect measurements using four different software programs. Besides the ability to use a specific computer software program for periodontal bone loss measurements, the use of digital images is advantageous due to the possibility of performing other bone loss analyses because digital images are easily obtained and can be used for radiographic interpretation.
Although a review of the literature shows that digital radiographic images of bone loss give an underestimation of measurements compared with the standard criterion,6,12,15,16 our results showed that digital radiographic images had the same results as the film-based images and direct visual measurement. According to a previously study,4 this result could be explained by the methodology used in our experiment: placing the periodontal probe accurately in the bone defect and following the root inclination with respect to the lower limit of the bone defect. The defects were created on the mesial side of the first pre-molar in the apical direction. This region was chosen because it was the area that offered the best access and provided a sufficient width to create a periodontal bone defect. One suggestion for further studies is to apply the same methodology in a clinical study.
In conclusion, periodontal bone defect measurements on an inverted digital image were inferior to film-based radiography and underestimated the amount of bone loss.



 XML Download
XML Download