

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Recently, patient exposure to medical and dental X-ray examination has grown rapidly and diagnostic radiology represents the largest source of artificial radiation which is comparable to natural background exposure.1 For patient protection, the principles of justification and optimization should be followed. All radiographic examinations have to show a potential benefit to the patient weighing against the potential risk. After they are justified, the radiographic exposure should be kept as low as reasonably achievable, taking into account economic and societal factors. The objective of this optimization is to decrease the total patient dose of radiation without compromising diagnosis. However, the optimization process is a complicated procedure. Many international and national surveys have shown a wide distribution of patient doses for the same type of radiographic examination.2 The concept of diagnostic reference levels (DRLs) has been introduced and applied to different radiodiagnostic examinations in the medical and dental field.2 DRLs are dose levels in medical radiodiagnostic practices for typical examinations for groups of standard-sized patients or standard phantoms for broadly defined types of equipment.3-5 These are based on the third quartile values for the distributions of doses found in the national or regional surveys, that is, 75% of hospitals are giving patient doses below these values. The 25% of hospitals above these are most urgently in need of better quality control, for example, identification of inadequate techniques or machine malfunctions.6
Dose quantities adopted for DRLs are patient entrance dose (PED), entrance surface dose (ESD), dose area product (DAP), and other dose-related quantities. PED is defined as the absorbed dose (to air) measured at the end of the spacer 'cone' for a typical examination (adult mandibular molar) without backscatter from the patient.6,7 ESD is defined as the absorbed dose to air at the point of intersection of the X-ray beam axis with the entrance surface of the patient, including backscattered radiation from the patient.8 DAP is defined as the absorbed dose to air averaged over the area of the X-ray beam in a plane perpendicular to the beam axis, multiplied by the area of the beam in the same plane, namely the integral of the dose across the X-ray beam.8 This is conveniently measured with special large-area ionization chambers (DAP meters), which intercept the entire cross section of the beam.8 DAP correlates reasonably well with radiation risk, as the number of interactions within the patient is proportional to both dose and field size.9 In dental radiology, PED was recommended and commonly used for the setting of DRLs, and it differs from the quantity ESD commonly used in general medical radiography by not including radiation backscattered from the patient.6,7 Recently, DAP has been recommended for the setting of DRLs in intraoral,8 panoramic,10,11 cephalometric,12 and cone-beam CT examinations.13
The objectives of this study were to survey the radiographic exposure parameters, and measure the patient dose for intraoral dental radiography nationwide, and thus to establish the DRLs in intraoral dental X-ray examination in South Korea. This was the first nationwide investigation for the development of DRLs in intraoral dental radiography. The patient doses were measured with both dose quantities, PED and DAP, in order to compare them with previous reports from other countries.
Materials and Methods
One hundred twenty-six intraoral dental radiographic machines in 95 dental institutions were selected from all regions of South Korea for this study. The radiographic exposure parameters for intraoral dental radiographic examination were surveyed with 126 intraoral dental radiographic machines. The patient doses were measured with a DAP meter (Diamentor M4-KDK, PTW, Freiburg, Germany) for 102 intraoral dental radiographic machines from March to October 2009 (Table 1). Due to the mechanical failure of the ionization chamber of the DAP meter, the last 24 radiographic machines were excluded from the patient dose measurement.
Radiographic exposure parameters (kV, mA, exposure time, focal spot-skin distance), size of hospital (university dental hospitals, dental hospital, dental clinic, public health center), type of image receptor system (film-based type, digital radiography type, computed radiography type), installation duration of machines (5 years or less, 6 years or more), and type of dental X-ray machine (wall-mounted fixed type, hand-held portable type) were documented. PED and DAP were measured three times at the end of the exit cone of the X-ray unit with a DAP meter for adult mandibular molar intraoral dental radiography (Fig. 1), and corrections were made for room temperature and pressure. The PED was expressed in terms of mGy and DAP in mGycm2. The measured PED and DAP were averaged and compared according to the size of hospital, type of image receptor system, installation duration, and type of dental X-ray machine. Independent t-tests and ANOVA tests were performed for the comparisons using SPSS 12.0.1 for Windows (SPSS Inc., Chicago, IL, USA).
Results
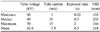
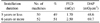
The ranges of exposure parameters for adult mandibular molar intraoral dental radiography were 60-70kV, 1-15mA, and 0.02-2 second and their means were 62.6 kV, 7.9 mA, and 0.5 seconds. The range of focal spot-skin distance (FSD) was 105-344 mm with a mean of 218mm (Table 2). In comparison of radiographic exposure parameters according to the size of hospital, the university dental hospitals showed the highest tube voltage and the shortest exposure time (Table 3). In comparison according to the type of image receptor system, the digital radiography (DR) type showed a higher tube voltage, lower tube current, and shorter exposure time than the film-based type (Table 4).
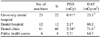
The mean patient doses were 2.11 mGy (PED) and 59.4 mGycm2 (DAP), and the third quartile ones were 3.07mGy (PED) and 87.4 mGycm2 (DAP) (Table 5, Figs. 2 and 3). The mean patient doses at the university dental hospitals were lower than those at the dental clinics (p<0.05) (Table 6). The mean patient doses of the DR type were lower than those of the film-based type (p<0.05) (Table 7). The mean patient doses did not show statistically significant differences according to equipment installation duration and type of dental X-ray system (Tables 8 and 9).
Discussion
National surveys on medical and dental radiography have been performed in many countries. Among them, the UK has reported national DRLs consistently through a series of five-yearly reviews of the National Patient Dose Database maintained by the Radiation Protection Division (RPD) of the Health Protection Agency (HPA).14 In the 2005 review, they reported that the reference doses were on average about 16% lower than the corresponding values in the previous (2000) review, and were typically less than half the values of the original UK national reference doses that were derived from a survey in the mid-1980s.14 The DRL for an adult mandibular molar intraoral radiograph recommended by the NRPB (the organization prior to the HPA in the UK) was 4 mGy in 19996,14 and it had fallen to 2.3 mGy at the next review in 2005.14 According to the IAEA Basic Safety Standards (1996),15 the guidance level of dose for periapical radiography was 7mGy(ESD). Pope et al5 carried out a comprehensive study in order to propose DRLs for intraoral radiology in Germany and reported the DAP value for mandibular molar radiographs to be 41.2 mGycm2. Tierris et al11 reported 62 mGycm2 (mean DAP) at 60 kV in Greece.
The 3rd quartile and mean values of the patient dose in the present study were 3.07 mGy and 2.11 mGy, respectively, in dose quantity of PED, and 87.4 mGycm2 and 59.4mGycm2, respectively, in dose quantity of DAP. From the measured patient dose values, we could observe a wide range in patient doses among different dental facilities, as has been reported in other countries.5,7 In our study, the range was from 0.21 to 10.98mGy, with a factor of around 50. The HPA report in the UK's 2005 review showed a much larger range from 0.02 to 30 mGy with a factor of 1500 between the lowest and the highest doses. It was reported that around 15% of dentists were using digital systems for intraoral radiography at that time in the UK.14 The 102 intraoral dental radiographic machines measured in this study comprised 43 of the film-based type, 56 DR type, and 3 CR type. Namely, about 58% of dentists used digital systems, particularly the DR type in Korea. The mean PED and DAP of the film-based type were 3.05mGy and 84.4 mGycm2, respectively, and those of the DR type 1.35 mGy and 38.8 mGycm2, respectively, which were much lower than the values for the film-based type. The reason why the mean patient dose in university dental hospitals was the lowest was concluded to be because they used radiographic equipment with a high tube voltage and sensitive DR sensor system. Film-based systems generally showed high patient doses. Although the mean patient dose of the DR systems was lower than that of the film-based systems, the DR systems showed a wide variation in doses among different models, from low to high patient doses (including some even higher than those of the film type). Therefore, when selecting an intraoral DR sensor system, a dentist should consider the patient dose as well as the image quality for the optimization of intraoral dental radiography.
In the comparison according to equipment installation duration, the machines 5 years or less showed a lower mean patient dose than those 6 years or more; however, the difference was not statistically significant. This was assumed to be because some newer DR systems showed a considerably high patient dose.
Fifteen hand-held, portable intraoral dental radiographic machines (15%) were involved in this study. In the comparison according to type of dental X-ray system, the mean patient dose of hand-held systems was slightly lower than that of the wall-mount fixed systems, but the difference was not statistically significant. This was believed to be because some hand-held systems showed a much higher patient dose than the wall-mount fixed systems. The use of hand-held dental X-ray systems for general dental radiography remains in dispute because its use requires the operator's hand holding the X-ray tube housing. In this nationwide survey, it was observed that most of them were combined with a DR sensor, but a few systems were combined with X-ray film. It is recommended that dental practitioners do not use a hand-held dental X-ray system if possible. In case its use is needed, they should select a hand-held dental X-ray system with a low patient dose and use it in combination with a sensitive DR sensor. This was the first nationwide survey for the development of DRLs for intraoral dental radiography in South Korea. Consistently reported DRLs will assist in the ongoing reduction of patient radiation doses.
In conclusion, we recommend 3.1 mGy (PED) and 87.4 mGycm2 (DAP) as the DRLs in adult mandibular molar intraoral dental radiography in South Korea based on this nationwide survey.









 XML Download
XML Download