

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ameloblastoma is the second most common odontogenic tumor.1 Ameloblastoma is a true neoplasm which is described as tumor that is usually unicentric, nonfunctional, intermittent in growth, anatomically benign and clinically persistent.2 Ameloblastoma is commonly a central lesion but rarely a peripheral epulis-like lesion.1
Based mainly on the clinical behaviour and prognosis, three types of ameloblastoma can presently be distinguished: (1) the 'conventional or classical', intraosseous, solid or multicystic ameloblastoma, (2) the unicystic ameloblastoma, and (3) the peripheral ameloblastoma.3 Recent studies could well indicate that desmoplastic ameloblastoma may be classified as a fourth subtype of ameloblastomas because of its biological behaviour, radiographic appearance, and unique histology.3 Several causative factors have been proposed, including (1) nonspecific irritating factors such as extraction, caries, trauma, infection, inflammation, or tooth eruption; (2) nutritional deficit disorders, and (3) viral pathogenesis.4
Among these types, intraosseous ameloblastoma is the most common and simple type encountered. Clinico-radiographically, intraosseous ameloblastoma presents as a painless swelling or slow expansion of the jaws, and it is described as multilocular expansile radiolucency that occurs most frequently in mandibular molar/ramus area. Peripheral ameloblastoma, a very rare pattern of ameloblastoma, generally occurs in the gingiva, and there is no bony involvement. It presents as a painless, sessile, firm, and exophytic growth that is usually relatively smooth or granular.5
Various cases of intraosseous ameloblastoma have been reported with the usual clinical presentation described above. In 1991, Kuru6 reported the first case of intraosseous ameloblastoma manifesting as a peripheral (exophytic) lesion. Later, two similar cases were reported by Tongdee and Ganggakavin7 and Stevenson and Austin8 respectively. As for our knowledge, this could be the fourth such a case to be reported in the English literature.
Case Report
A 45-year-old male patient reported with a gingival growth on the right anterior region of the mandible for one year and also complained of pain in the same region for 6 to 7 months. The exophytic lesion was small initially and increased gradually to the current size displacing the adjacent teeth. He had mild and intermittent pain. He had visited a dentist with the same complaint 7 months before. His general physical status was normal. Extraorally, a diffuse swelling measuring around 1.5×1.5 cm in size was seen on the right lower portion of the face. The skin over the swelling was normal and was tender on palpation.
Intraoral examination revealed an exophytic lesion on the right mandible (Fig. 1A) at the interdental gingiva between canine and the first premolar, which was roughly circular, measuring about 3.5×3.5 cm in size, extended labially from the attached gingiva to the lingual sulcus of the right mandibular incisors, canine, and premolar. The surface of the lesion (Fig. 1B) was pebbled and rough with indentations of the opposing teeth with mesially displaced canine. Color of the lesion was normal as that of the surrounding mucosa and firm in consistency. The associated teeth were vital but tender, and grade I mobility was present. No cortical expansion was found.
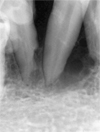
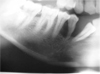
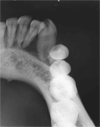
The periapical digital radiograph (Fig. 2) showed the presence of characteristic multilocular soap bubble appearance in the region of canine and first premolar, and knife edge shaped root resorption pattern in relation to the first premolar. The panoramic radiograph (Fig. 3) showed radiolucency measuring 4×4 cm in diameter extending from the distal aspect of lateral incisor to the mesial aspect of second premolar. The occlusal radiograph (Fig. 4) showed no expansion of the cortex. Blood investigations were within normal limits and serum chemistry showed no significant changes. The lesion was surgically removed (Fig. 5) and was subjected for microscopic examination (Fig. 6) which revealed normal stratified squamous epithelium which was parakeratinized. Connective tissue showed follicles which were arranged in various sizes and shapes. The follicles were lined by a single layer of tall columnar ameloblast-like cells and little cystic degeneration. Continuity of the tumor cells with epithelium was not evident. These features were suggestive of amelobalstoma (follicular type).
Discussion
Ameloblastoma usually manifests as an intraosseous or central lesion or rarely as a peripheral epulis-like lesion.1 The lesion may arise most commonly from cell rests of enamel organ, epithelium of odontogenic cysts, disturbances of the developing enamel organ, and basal cells of oral epithelium. Clinico-radiographically, ameloblastoma can be divided into 3 distinct patterns: (1) the conventional solid/multicystic (86% of all cases), (2) the unicystic (13% of all cases), and (3) the peripheral (1% of all cases) (extraosseous).2
Various histologic forms have been described which include follicular, plexiform, acanthomatous, granular cell, desmoplastic, and basal cell patterns.2 Follicular ameloblastoma presents as a painless swelling or slow expansion of the jaws, and it is described as multilocular expansile radiolucency that occurs most frequently in mandibular molar/ramus area.9 Desmoplastic variant occurs more frequently in the anterior mandibular region10 and presents a mixed radiopaque and radiolucent appearance. Unicystic ameloblastoma is usually seen in younger age and most commonly associated with pericoronal radiolucency with unerupted 3rd molar (38%).11
In this particular case, the clinical presentation of the follicular ameloblastoma was different from the usual presentation, which included exophytic growth, uncommon location, and absence of expansion of the cortex. The lesion had started intraosseously, however eventually perforated to involve the soft tissue. Clinically differential diagnosis of this exophytic growth included peripheral ameloblastoma, peripheral odontogenic fibroma, peripheral giant cell granuloma, and other peripheral hyperplastic swellings superficial to the alveolar ridge.9 The final diagnosis was made by the clinical, radiological, and histopathological features after the complete excision of the lesion.
Kuru first reported an intraosseous ameloblastoma having penetrated through the alveolar bone, fused with the oral epithelium, and eventually presenting itself clinically as a 'peripheral lesion'.6 Our case had the similar clinical and radiological features of the previously reported case by Kuru but with no expansion of the cortex. Two other similar cases have been reported by Tongdee and Ganggakavin7 in 1978 and Stevenson and Austin8 in 1990, respectively. The exophytic growth is also a characteristic finding of the peripheral (extraosseous) ameloblastoma which is very rare. Radiographically, or at surgery, a superficial erosion of the bone or a superficial bony depression -known as cupping or saucerization- may be noticed, a finding that is thought to be due to pressure resorption, in contrast to resorption caused by neoplastic invasion.5 The diagnostic criteria of peripheral ameloblastoma include the origin from the overlying epithelium, presence of odontogenic epithelium islands in the lesion, and lack of potential to bone infiltration.12 Also, peripheral odontogenic fibroma and peripheral giant-cell granuloma share the same clinical characteristic of exophytic growth most commonly at mandibular premolar region, despite the histopathological difference. However, radiographically, both of them create depression/resorption in the underlying bone very rarely.13
Most oral surgeons and pathologists unquestionably consider peripheral ameloblastoma to be a nonaggressive lesion without actual infiltration into the underlying bone.14 One of the main problems regarding peripheral ameloblastoma is its possible origin. The two main theories are the following: (1) origin from the extra osseous epithelial remnants of dental lamina and its organ derivatives within the underlying connective tissue; (2) origin from the basal cell layer of the oral mucosa, which is believed to have odontogenic potential.15 Those lesions that are entirely separated from the overlying surface epithelium probably arise from the odontogenic remnants, however this hypothesis can be questioned if there is continuity between the tumor and the surface epithelium.
In conclusion, even though the incidence of intraosseous ameloblastoma manifesting as exophytic lesion is very rare, it may have to be considered in the differential diagnosis of exophytic lesions at the region of mandibular canine premolar region along with peripheral ameloblastoma, peripheral odontogenic fibroma, peripheral giant cell granuloma, and rarely peripheral hyperplastic swellings superficial to the alveolar ridge.



 XML Download
XML Download