

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ameloblastomas, although locally invasive, are considered to be benign neoplasms derived from odontogenic epithelium. The term "ameloblastoma" includes several clinico-radiographic and histological types. Based on the clinical behavior and prognosis, three types of ameloblastomas can be presently distinguished: (1) the 'conventional or classical', intraosseous, solid or multicystic ameloblastoma; (2) the unicystic ameloblastoma; and (3) the peripheral ameloblastoma.1 Recent studies could well indicate that the desmoplastic ameloblastoma might be qualified as a fourth subtype of ameloblastomas because of its biological behavior, radiographic appearance, and unique histology.2
In 1977 Robinson and Martinez3 described unicystic ameloblastoma as a distinct variant of ameloblastoma with a large cystic cavity showing either mural or luminal proliferation of ameloblastic tumor cells. Histologically, this variant is sub- divided into four different types4,5 among which, the types showing mural growth requires aggressive treatment because of their behavior.6 Eversole et al7 in 1984 described a new type of ameloblastoma which presented a unique histopathological pattern and clinico-radiographic findings. Histologically, it was characterized by extensive stromal collagenization or desmoplasia with small nests and strands of odontogenic epithelium, which was later designated as desmoplastic ameloblastoma.8
'Hybrid lesion of ameloblastoma' was first described by Waldron and el-Mofty8 in 1987 and is one of the variants of ameloblastoma, in which, histologically, areas typical of classic follicular or plexiform ameloblastoma coexist with areas characteristic of desmoplastic ameloblastoma. The biological profile of this variant has not been clear, due to the lack of adequate case reports published so far.8-12
Here we report a distinctive case of unicystic ameloblastoma of right mandible with unusual mural histopathological findings, where follicular and acanthomatous ameloblastoma-like areas were admixed with desmoplastic ameloblastoma like areas, similar to that of so-called hybrid lesion of ameloblastoma.
Case report
A 46-year-old male patient was referred to Dayananda Sagar Dental College and Hospital with a gradually enlarging swelling of the right mandible crossing the midline. The patient had noticed the tumor 5 years before and enlargement of the tumor 4 months prior to admission. Physical examination revealed a swelling on the right mandibular angle area. Intraorally, a bony hard painless swelling was extending from the lower right third molar region to the left canine region with intact overlying mucosa. All the teeth in the lesional area were vital with mobility of the right incisors and molars.
The panoramic radiograph revealed a predominantly well defined multilocular radiolucency with sclerotic border and scalloped margins in the right mandibular body region. Antero-posteriorly, it extended from the mesial aspect of third molar region to the mesial aspect of first premolar and superior-inferiorly from the periapical region of the right mandibular posterior teeth to the inferior body of the mandible. Anterior to the multilocular radiolucency, an area of mixed radiopaque/radiolucency was noted extending from the mandibular right second premolar to the mandibular left lateral incisor crossing the midline. The entire lesion measured about 8×4 cm. Root resorption of lower anterior teeth and molars were noticeable (Fig. 1). Axial computed tomograph (CT) revealed a mixed radiolucent-radiopaque mass with well defined borders on the right mandibular body crossing the midline along with buccal cortical plate expansion (Fig. 2).
Based on the clinical and radiographic findings a presumptive diagnosis of ameloblastoma or odontogenic keratocyst was made. Incisional biopsy was performed from the posterior and anterior regions which were submitted to the department of oral pathology. The biopsy from the posterior region was reported as a unicystic ameloblastoma of mural type and the biopsy from the anterior region was reported as a follicular ameloblastoma with acanthomatous changes. A hemi-mandibulectomy was performed for tumor resection under general anesthesia. The resected specimen measured about 9×4×2 cm (Fig. 3). The tumor was solid with few cystic areas, and the cut surface was slightly brown.
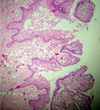
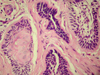
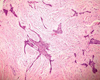
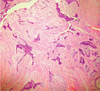
Multiple histological sections were prepared from the resected mandible representing all the areas and were thoroughly analyzed. The main part of the tumor showed cystic lining of ameloblast-like cells, which were tall columnar, having peripheral palisading and hyperchromatic nuclei. Intra luminal proliferations of ameloblast-like cells were found in plexiform pattern (Fig. 4). The mural part of the tumor mass showed follicular and acanthomatous ameloblastoma, which coexisted with desmoplastic ameloblastoma (Figs. 5 and 6). This association of desmoplastic ameloblastoma with follicular and acanthomatous patterns, was consistent with the features of so-called hybrid lesion of ameloblastoma (Fig. 7). The final diagnosis of 'Unicystic Ameloblastoma type 1.2.3 - luminal, intra luminal, and intra mural type' was made.
Discussion
Ameloblastoma is a benign odontogenic neoplasm that frequently affects the mandible. The term ameloblastoma includes several clinico-radiological and histological types.1 Apart from the most commonly encountered clinico-pathologic models, there are few variants, whose biological profile is unknown or not elicited. The fact is the scarcity of such case reports published till date.5,9
The unicystic ameloblastoma is a distinctive type of ameloblastoma, which has been sub-grouped into four different entities. They are luminal (1), luminal and intra luminal (1.2), luminal, intra luminal, and intra mural (1.2.3), luminal and intramural (1.3) types.4,5 Among these types, unicystic ameloblastomas showing mural proliferation are considered invariably aggressive and should be treated in the same manner as solid multicystic ameloblastoma, whereas other variants can be treated conservatively.4-6
The desmoplastic ameloblastoma is a rarely encountered type of ameloblastoma with different biological behavior than that of conventional ameloblastoma. It is identified histologically, by irregular odontogenic islands with a stretched out kite-tail appearance in a dense desmoplastic stroma.13 Occasionally, desmoplastic ameloblastoma shows large tumor islands exhibiting bizarre appearance with typical animal like configuration.5
The radiographic features of conventional ameloblastoma are classified as unilocular or multilocular radiolucencies with well defined borders. The radiographic features of desmoplastic ameloblastoma differ from that of conventional ameloblastoma to a great extent. The desmoplastic ameloblastoma usually shows mixed radiolucent/radiopaque areas with ill-defined borders similar to that of fibroosseous lesions.9 In a review of 115 cases of desmoplastic ameloblastomas by Sun et al,14 55.6% of desmoplastic ameloblastomas showed mixed radiolucent/radiopaque areas with poorly defined borders. In a case report of hybrid ameloblastoma by Wakoh et al,15 the lesion consisted of a mixed radiolucent/radiopaque area with an adjacent cystic radiolucent area. The mixed area was seen in the mandibular anterior region and cystic radiolucent area was inferior to the apex of second premolar. In the present case, similar radiographic findings were noticed, where mixed radiolucent/radiopaque area was adjacent and anterior to a well defined multilocular radiolucent area. In most of the cases of desmoplastic ameloblastoma new bone formation has been reported, which explains the mixed radiolucent/radiopacities.9
The histopathological diagnosis of present case was unicystic ameloblastoma of luminal, intra-luminal and intra-mural type (1.2.3). The cystic lining of lumen was lined by ameloblastic epithelium showing hyperchromatic, polarized basal cell layer. The overlying epithelial cells were loosely cohesive resembling stellate reticulum like cells. The intra luminal proliferation was in plexiform pattern, similar to that of plexiform unicystic ameloblastoma, a histological pattern explained by Gardner16 in 1981. The mural histopathology was bit unusual, which showed follicular and acanthomatous areas coexisting with desmoplastic areas. The follicular type of ameloblastomatous islands were showing stellate reticulum kind of cells in the center, surrounded by tall columnar cells peripherally, with palisading, hyperchromatic nuclei. Few follicles showed squamous metaplasia of centrally located stellate cells, quite similar to acanthomatous ameloblastoma. The much of connective tissue stroma was fibrous, admixed with few areas of pronounced desmoplasia, with thick collagen fibers. The tumor islands in these desmoplastic areas seemed to be compressed from the periphery by dense bundles of collagen fibers, to give a stretched out kite-tail appearance. Few islands were bizarre with 'animal-like' configuration. This pattern was comparable with desmoplastic ameloblastoma, described first by Eversole et al in 1984.5, 7,13
Waldron and el-Mofty in 1987, first described 'hybrid lesion of ameloblastoma' another tumor variant, in which, histologically, areas of follicular or plexiform ameloblastoma coexist with areas characteristic of desmoplastic ameloblastoma.8 The present case showed a similar mural picture, in which areas of follicular and acanthomatous ameloblastomas were admixed with areas of desmoplastic ameloblastoma. This blend of different clinico-pathologic ameloblastomas was highlighted by Philipsen et al,9 in a review of 100 cases of desmoplastic ameloblastoma. They mentioned about nine cases of hybrid lesions of ameloblastoma in the literature review. The authors did not elicited the biological profile of this 'hybrid lesion of ameloblastoma' because of the lack of such cases with detailed clinical, radiological data and corresponding histopathological analysis.5 They recommended treating these cases like other variants of infiltrative ameloblastomas till the biological behavior was clarified.9
Most of the reported cases of mural proliferations have been either a plexiform, follicular or a mixture of the above two patterns. However, rarely do, we found a combination of follicular, acanthomatous, and desmoplastic areas in one lesion. The mural picture of the present case demonstrates a rare mixture of all these various patterns in a single lesion, similar to the case of hybrid ameloblastoma reported by Hirota et al, in which desmoplastic areas were associated with follicular, plexiform, acanthomatous, and basal cell ameloblastoma.17
The patient's age in our case, corresponded more with the conventional ameloblastoma than with the unicystic ameloblastoma, which the unicystic changes might be secondary in a long standing solid multicystic ameloblastoma, due to the cystic degeneration of stellate reticulum like cells and subsequent fusion of the ameloblastic follicles as suggested by Leider et al.18 It was not clear whether desmoplastic changes occurred secondary in the stroma of a pre-existing solid-multicystic ameloblastoma or whether a part of primary desmoplastic ameloblastoma altered into conventional ameloblastoma or whether the 'hybrid' lesion was a kind of collision tumor.8,12 The focal proliferation of fibrous connective tissue seen in the present case could be ascribed to mesenchymal induction mediated by few focal neoplastic ameloblast-like cells.19
The radiographic features of the present case, was showing combination of two typical radiological appearances, which consisted of mixed radiolucent/radiopaque areas (suggestive of desmoplastic ameloblastoma) adjacent to multilocular radiolucent area (suggestive of conventional ameloblastoma). This feature may become a radiological clue towards the diagnosis of so-called 'hybrid lesion of ameloblastoma'.
Our case was unicystic ameloblastoma with diverse mural proliferation associated with areas resembling desmoplastic ameloblastoma, however the term 'hybrid ameloblastoma' has been designated only for conventional ameloblastoma associated with desmoplastic ameloblastoma. If this term 'hybrid' can expanded for unicystic ameloblastoma with diverse proliferation, then the present case may become another addition to reported cases of so-called hybrid lesion of ameloblastoma.
The average duration of follow-up for ameloblastomas in previous reports was 5 years after the surgical treatment. Recurrence rate of 53% was found during the first five years.19 In the present case, no recurrence has been observed from past two years.



 XML Download
XML Download