

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Head and neck infection initially spreads to oral vestibule or myofascial space. However, if such initial infection progresses and spreads near the pharynx, airway obstruction may occur and it can cause death in serious cases. If infection spreads to the carotid sheath, the damaged vessel may cause bleeding or nerve disorder.1,2 Contrast-enhanced computed tomography in an appropriate phase helps the diagnosis of the infection and its spreading route, leading to successful treatment. If infection spreads to the retropharyngeal space, it progresses quickly through the superior and posterior to the mediatinum causing severe complications and the progress may continue on to the prevertebral space, diaphragm, and thorax. Even with antibiotics and surgical treatment, mediastinitis is a severe complication with 35-50% of fatality rate. Also, if the infection spreads in the superficial level, necrotizing fasciitis may occur and it can cause gangrenes on the skin and its following complications such as systemic shock. Therefore, the early diagnosis of infection and appropriate treatment is very important in head and neck infections.
In this report, we introduce a patient with extensive chronic mandibular osteomyelitis with necrotizing fasciitis and airway obstruction by deep neck infection in the lateral pharyngeal space, subscapular space, and carotid sheath, who was successfully treated by early diagnosis, continuous incision and drainage, active antibiotic treatment and follow up dressing through the appropriate use of radiographic images, along with a review of literature.
Case Report
A 77-year-old female visited our clinic with a chief complaint of painful swelling in the submental area which had begun 2 days ago. The patient had been treated for pulmonary edema caused by asthma and aspiration pneumonia from 7 years ago, and she was currently being treated for pyelitis, cerebral infarction, dementia and herpes zoster. Clinical examination showed several root rests, gingival swelling on the entire dentition, redness and pus discharge in the upper and lower anterior teeth, induration, redness, and tenderness to palpation on the submental area. Also, bilateral bone exposure on the lingual mandible suggested osteomyelitis. Trismus, dysphasia and dyspnea were not found.
On the initial visit, clinical and radiographic examinations including panoramic radiograph were carried out. On the panoramic radiograph, several dental caries were observed, as well as periapical abscess on the right maxillary lateral incisor and right maxillary first molar. Extraction sockets were also observed. Ill-defined bony destructive change on the left mandibular canine area with sclerotic change of surrounding trabecular bone was found (Fig. 1). The patient was tentatively diagnosed with submental space abscess. Incision and drainage was carried out under local anesthesia and a drain was inserted lingually, however pus drainage was poor.
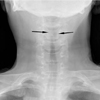
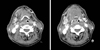
On the next day, dysphasia and dyspnea were intensified. Soft tissue neck anteroposterior view and oxygen saturation was examined. On the radiographic image, the airway was severely narrowed (Fig. 2). The oxygen saturation was 89%. Immediate endotracheal intubation was carried out and the oxygen saturation was stabilized at 96%, with no other problem on vital sign. Blood test revealed high inflammation values with white blood cell at 18,110/mm3 and C-reactive protein at 33.23 mg/dL. Infusion and antibiotic treatment (amoxicillin-potassium clavulanate, isepamicin sulfate, and metronidazole) was carried out. Contrast-enhanced CT images showed non-enhanced low attenuated region with the irregular periphery of non-homogeneous enhancement on the right submandibular space (Fig. 3). Also, these findings were found similarly in the bilateral submental and the left submandibular spaces. There was enhanced soft tissue swelling in the nasopharynx, oropharynx, and the inferior pharynx. The airway was deviated to the left and had decreased diameter. Extraoral incision and drainage on the submental area was immediately carried out under general anesthesia. Necrotizing fasciitis was suspected, and the necrotized area was removed. Drains were inserted in bilateral submandibular and submental area. The patient was transferred to the intensive care unit without removing the endotracheal tube.
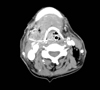
After surgery, saline with povidone-iodine irrigation in the drain insertion area was carried out twice a day. The necrotizing area in the submental region was increased. Blood test revealed that there was no difference in the inflammation level. However, the follow-up contrast-enhanced CT revealed that pus had spread widely to the posterior area of the right sternocleidomastoid muscle, retropharyngeal space, parapharyngeal space, hyoid bone area, and prevertebral space (Fig. 4). Due to the increasing necrotizing area and the deep spread of the infection, the previous drains were removed and further submental necrotized area was excised under general anesthesia. An incision was made 6 cm below the anterior border of the right sternocleidomastoid muscle, and the pus formation space was reached and irrigated. Drains were inserted from the superior border of the left clavicle to the left mandibular border, from the submental area to intraoral area and to the right mandible border, and from the anterior border of the right sternocleidomastoid muscle to the interclavicular area. Intraoral drains were inserted in the right submandibular area and in the right pterygomandibular space.
After the second surgery, saline with povidone-iodine irrigation in the drain insertion areas was continued twice a day. Another follow-up contrast-enhanced CT showed reduced pus formation in the submental area, right parapharyngeal space, and retropharyngeal space. Blood test resulted in decreased inflammation, however the edema in the airway and the pus formation around the hyoid bone were still found. Third surgery was carried out under general anesthesia. The drain in the right sternocleidomastoid muscle area was removed. An incision was made on the hyoid bone area. When the hyoid bone was completely reached, a small amount of pus discharge was observed. After vigorous irrigation, additional drains were inserted in the right sternocleidomastoid muscle incision area in the direction of the hyoid bone, the interclavicular area and above the right clavicle. After surgery, the drains were irrigated with saline mixed with antibiotics (Ceftriaxone 1 g, Hanmi Pharm, Seoul, Korea) twice a day. The other follow-up contrast-enhanced CT (Fig. 5) showed that pus formation in the right submandibular and submental area had almost completely disappeared, as well as the parapharyngeal and the retropharyngeal space. The edema in the airway was also reduced, therefore the endotracheal tube was removed. The patient state was stabilized and she was transferred to the general ward.
The number of the drains was reduced as the patient's state improved. Blood test revealed decreasing inflammation state. The frequency of irrigation on the drain area reduced to once a day. Appointment for treatment plans regarding the mandibular osteomyelitis that was observed on the follow-up CT was scheduled.
Discussion
Among odontogenic infections that lead to deep space abscess, mediastinitis and necrotizing fasciitis of the neck are known to be secondary complications which can be life threatening. Patients with odontogenic infection who require incision and drainage in the oral maxillofacial region are normally affected with more than one myofascial space. Generally, submandibular, submental, and parapharyngeal space are affected.3 When head and neck infection spreads to the fascia and the subcutaneous tissue, necrotizing fasciitis may occur and sometimes follow a deeper infection path. The more caudal the infection spreads, the more likely the severe complications such as mediastinitis may occur.
Necrotizing fasciitis of head and neck is caused by infection of several fatal bacteria. Infection spreads along the fascia and affects the subcutaneous tissues, myofascia, skin and muscles.4 This type of infection is very rare in head and neck region and odontogenic infection causes it even rarer. If immediate treatment is not applied, the infection spreads quickly and becomes fatal. The fatality rate was reported to be 20-75%.5 Deep neck infection can also arise from infections of the teeth, glands, and neck lymph nodes, however odontogenic causes are few.6 Such infections spread to the parapharyngeal and retropharyngeal space to obstruct the airway, or take an upper path to form brain abscess, or when it spreads along the carotid sheath, fatal long-term complications such as bleeding due to vessel damage may occur. Bonapart et al7 stated that the main routes of neck infection spreading to the mediastinum were the prevertebral space, which connected to the anterior part of the mediastinum, and the retropharyngeal and viscerovascular space, which lead to the posterior part of the mediastinum and the diaphragm. In this report, the infection had spread to the parapharyngeal space and the prevertebral space, but not to the mediastinum.
For evaluation of deep neck space infection, ultrasound, MRI, and radiographic examinations such as soft tissue neck X-ray, CT may be useful. The soft tissue neck X-ray is the most convenient method, and it is especially useful for evaluating the retropharyngeal space and the prevertebral space since it allows the measurement between the anterior part of the vertebrae and the posterior wall of the pharynx. In the present case, when the patient was displaying dyspnea, the soft tissue neck anteroposterior view allowed the evaluation of the airway obstruction and its following treatment. However, using the soft tissue neck X-ray alone for the diagnosis, gives 33% of false negative rate, meaning that other imaging evaluation method is required for a more accurate clinical diagnosis.8
Ultrasonography has been used to detect abscess cavities, although the anatomic detail provided by CT makes it superior in confirming the presence of an abscess.9 MRI can provide more detailed anatomic structures, and can detect infected spaces which have been indefinable on CT images. However, the high cost, time for image processing, and the cooperation required from the patients are the disadvantages.10
Contrast-enhanced CT images clearly delineate the position and size of the lesion as well as its relationship with the adjacent anatomic structures. Also, it is useful in evaluating any changes in the upper airway in patients with trismus or with parapharyngeal or retropharyngeal space abscess. The images provide valuable information in deciding the method for maintaining the airway such as endotracheal intubation, cricothryoidotomy, or tracheostomy.11 On CT images, the attenuation level of space abscess is between that of water and soft tissues. When a contrast medium is used, a rim enhancement around the abscess area is observed. Swelling of the adjacent muscles signifies the spreading of inflammation in the surrounding area.12 In the present case, the contrast-enhanced CT was used to identify the spreading of pus into deeper spaces after initial treatment, and for guiding extensive incision and drainage under general anesthesia to prevent further expansion. Also, follow-up CTs were used to evaluate the edema of the airway and to determine the timing for endotracheal extubation.
For effective treatment of deep space abscess, early accurate diagnosis and its appropriate treatment mandatory, and for necrotizing fasciitis, absolute understanding of the anatomical structures in the infection area and active surgical treatment along with intensive antibiotic treatment is necessary.
In our case, since the patient state was in severe, the urgent infection was treated with antibiotics for a long term, and sequestrectomy and decortication of the exposed bone in the oral cavity was sufficient for satisfying results instead of extensive mandibulectomy.
In conclusion, early diagnosis and treatment is important for a good prognosis of deep neck infection. When the infection spreads to the deep neck area, especially contrast-enhanced CT would be useful to observe every fascial space and to locate abscesses effectively in the head and neck area.


 XML Download
XML Download