

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
External apical root resorption (EARR) is an undesirable consequence of orthodontic treatment. The pathogenesis is associated with the removal of necrotic tissue from the areas of the periodontal ligament that has been compressed by an orthodontic load.1-3 Because cementum is normally more resistant than bone, orthodontic forces to a tooth usually cause bone resorption rather than the loss of cementum. Root resorption occurs when the pressure on the cementum exceeds its reparative capacity and dentin is exposed, allowing the multinucleated odontoclasts to degrade the root substance.4
Although the relationship of orthodontic treatment with root resorption has been studied extensively,5 the factors related to the EARR were not clearly understood because no human studies on EARR could be performed in prospective randomized clinical trials due to the ethical considerations.6 Consequently, the previous studies differed significantly in terms of their study designs, methodologies, types of controls, and treatment assignments.6 Therefore, it was difficult to compare the results with the conclusions.7 The purpose of this study was to examine the patient- and treatment-related etiologic factors of EARR retrospectively.
Materials and Methods
This study consisted of patients who had completed orthodontic treatment at the Department of Orthodontics, Pusan National University. The selection criteria were as follows; the existence of complete records of the malocclusion; treatment plan and treatment history; a pre- and post-treatment panoramic radiograph taken within 1 month of debonding; and a pre- and post-treatment lateral cephalometric radiographs using a cephalometric radiography equipment (PM2002CC, Planmeca, Helsinki, Finland) with a standardized technique. The dental records were reviewed and the patients with a history of systemic illness, craniofacial abnormalities, tooth injury, endodontically treated teeth, or impacted teeth were excluded from the study.
One thousand patients' files were reviewed. Of these, 207 patients satisfied the selection criteria. The cases which the apices could not be accurately visualized were excluded. The cases that increased in the length of tooth due to the cosmetic reshaping of the incisal edge were also excluded. Finally, 163 patients were included in the study.
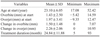
Table 1 shows the distributions of the samples. The final study group included 163 patients with the age range of 17.1-52.4 years at the initiation of the treatment. Overbite and overjet were measured with the pre- and post-treatment lateral cephalometric radiographs to calculate the changes in overbite and overjet. Of the 163 patients, 78 patients were treated with extractions and 85 without extraction. The duration of their orthodontic treatment ranged from 5 to 93 months (Table 2).
Root resorption measurement
The tooth length from the tooth apex to incisal edge or cusp tip was measured on the panoramic radiograph using a digital caliper (accurate to 0.01 mm). These measurements were performed on both pre- and post-treatment panoramic images. Root resorption was calculated by the difference of the tooth length between the images.
The tooth length was measured for the left and right permanent second premolars, canines, lateral incisors, and central incisors on both jaws. Only teeth which had completed the root formation were measured. This radiographic measurement was then converted to the actual length considering the enlargement ratio 1.2.
The measurement error of the tooth length was analyzed using the intra-observer reproducibility of 40 randomly selected panoramic radiographs; 20 radiographs taken before orthodontic treatment and the corresponding 20 ones at the end of active treatment. The tooth length was re-measured one month after the original measurements. The paired t test showed no significant difference between the first and second measurement.
Data analysis
The root resorption was calculated by subtracting the post-treatment values from pre-treatment values. The root resorption of the tooth and the factors of malocclusion were analyzed with an one-way ANOVA. An independent t test was performed to compare the mean amount of resorption between male and female, between extraction and non-extraction cases, and between surgery and non-surgery groups. The correlation coefficients were measured between the amount of root resorption and the beginning age of the orthodontic treatment, changes in overbite, and overjet and the duration of treatment. The statistical analyses were carried out using SPSS (ver. 13.0 for Windows, Chicago, IL, USA).
Results
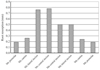
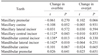
There was no significant difference of root resorption between the right and left sides. The maxillary central incisor was the most resorbed, followed by the maxillary lateral incisor, the mandibular central incisor, and the mandibular lateral incisor. There were significant differences in the severity of root resorption according to the tooth types (Fig. 1). Significant correlations between the change in overbite and the amount of root resorption were found in maxillary and mandibular central incisors and mandibular lateral incisors. For overjet, there was no significant correlation (Table 3). Openbite cases showed more root resorption for maxillary and mandibular central incisors, and mandibular lateral incisors (Table 4). Gender, beginning age of the treatment, and Angle's classification were not statistically related with root resorption.
A history of tooth extraction was significantly related with post-treatment root resorption (Table 5). The duration of orthodontic treatment was positively correlated with the amount of root resorption (P<0.01, Table 6). The orthognathic surgery did not show statistically significant correlation with root resorption.
Discussion
EARR is commonly caused by orthodontic treatment. The description and analysis of EARR extends throughout this century, however few variables are clinically valuable as predictors of EARR because of the large inter-individual variations in response to treatment.8 The purpose of this study was to investigate whether the patient- and treatment-related factors were related to the amount of root resorption.
The root length could be measured from the apex to the midpoint of cementoenamel junction (CEJ) in order to evaluate the root resorption, however this method could cause greater variance.9,10 The errors in defining the point could probably make the inaccuracy,11 therefore the difference of the total tooth length was measured for evaluating the amount of root resorption in this study.
Harris reported that the risk of EARR also seemed to be independent of the age once the root formation had completed.8 The traditional concept that the orthodontic rootresorption increased with age4,12-14 was recently disproved.15-17 In agreement with these recent reports, our study also showed no relationship between the patient's age and the amount of resorption.
In general, the types of tooth which are moved the farthest tend to show the most frequent and severe EARR.18-20 The maxillary incisors are generally, on average, moved a greater distances during treatment than other teeth. It was reported that the incisors were most likely to show EARR and the severest resorption.21,22 Regardless of the genetic or treatment-related factors, the maxillary incisors consistently showed more apical root resorption than any other teeth.20,23-25 In this study, the maxillary central incisors were the most resorbed and the frequency of EARR over 1 mm after treatment ranged from 27% in the maxillary central incisors, where as it was 2% in the maxillary premolars.
The possible correlation between the duration of active treatment and the incidence and severity of EARR was controversial.16,20,25-29 Some studies concluded that the duration of treatment might be correlated to the extent of EARR,19,22,30 while others found no significant association between EARR and treatment duration.28,31 The duration of treatment was the most often correlated with the apical root resorption in meta analysis of the treatment-related factors of external apical root resorption.6 Our study revealed that the duration of treatment was significantly correlated with the root resorption. The longer treatment might reflect more severe malocclusion and/or different treatment mechanics.19 However, it should be considered that the amount of tooth movement was not a direct function of the duration of treatment. Confounding variables such as the more difficult treatment plans, appointment intervals, or lack of patient cooperation might cause the longer treatment time and also relate to EARR.32
Sharpe et al19 showed that the incisors experienced more EARR in extraction cases of premolars in which the retraction was greater than in non-extraction cases. The incidence of EARR was 3.72 times higher in patients for whom extractions were performed than those without extraction.17 In this study, the extraction cases demonstrated relatively more EARR compared with the non-extraction cases. Also, the patients with extraction of their teeth requested the longer treatment time to finish their orthodontic treatment. It could be supposed that the extraction of teeth could increase the amount of movement and treatment duration.
Harris and Butler33 documented that in the sample of cases with anterior open bites, the larger the overjet, the greater risk and degree of root resorption during the treatment. More incisor resorption was observed in the cases with larger overjet and overbite.31 In our study, although openbite cases showed more root resorption in mandibular central incisors, deepbite cases had lesser root resorption. In contrast to other studies,12,31 our study revealed no correlation between the amount of overjet at the beginning of treatment and the amount of root resorption.
In conclusion, the patient- and treatment-related variables and their relationship to the apical root resorption were as follows in this study. Neither the gender nor the age of the patient was related to the degree of resorption. The maxillary central incisors were the most resorbed teeth, with 27% undergoing greater than 1 mm of root resorption and premolars and canines were relatively unaffected. Increased openbite was weakly correlated with more root resorption in maxillary and mandibular central incisors and mandibular lateral incisors. The duration of treatment was significantly related to the amount of root resorption. There was difference between extraction and non-extraction therapy for root resorption.




 XML Download
XML Download