

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intraoral periapical radiography is useful in most of dental procedures. The main indications for this technique include detection of dental caries, periapical pathologies, assessment of periodontal status, assessment of root morphology before extractions and during endodontic procedures, trauma to teeth and the associated structures, and assessment for implant surgery. There are some patients with problems during intraoral periapical radiographic examinations including their age, anatomical difficulties like large tongue, shallow palate, restricted mouth opening, neurological difficulties, and so on. Thus a large group of patients are unable to tolerate the intraoral film/sensor placement in their mouth.1 The number of these patients is increased in size with the advent of digital radiography because of the rigidity and thickness of the radiographic sensor.2 For these patients, Newman and Friedman in 2003 developed an alternative technique for treating a wide spectrum of patients who could not tolerate intraoral placement of film.3 However, they reported the use of extraoral technique only during endodontic procedures. Later Chen et al in 2007 developed a sensor beam alignment aiming device for performing radiographs using this technique.4
Until now there have been very limited literatures documenting the use of this technique. Here we present various cases that this alternative technique was used for taking radiographs. This technique was used to take radiographs of patients during endodontic treatment, for pediatric patients, and for taking radiographs of impacted third molars.
Materials and Methods
The extraoral periapical radiographic technique was performed for both maxillary and mandibular teeth using Newman and Friedman technique.2
Maxilla (Fig. 1A): The patient was positioned upright, with his/her mouth was opened as wide as possible, to allow the X-ray beam to pass to the sensor unobstructed from the opposite side of the mouth. The sensor was placed on the external surface of the cheek, directly buccal to the tooth. A cotton roll was placed between the sensor and the cheek to parallel the sensor with the buccal surface of the tooth. The X-ray cone was angled approximately -25 degrees from the horizontal plane. Additionally, the X-ray beam was aligned perpendicular to the sensor to provide an accurate image.
Mandible (Fig. 1B): The patient was positioned upright with raised chin, which allowed the X-ray beam to reach the sensor unobstructed. The sensor was placed on the external surface of the cheek, directly buccal to the tooth. The X-ray cone was angled approximately -15 degrees from the horizontal plane. Additionally, the X-ray beam was aligned perpendicular to the sensor to provide an accurate image.2
The images were obtained using Sopro digital imaging system (Acteon Group, Marseills, France) and a 30×40 mm standard intraoral sensor SOPIX (Acteon Group, Marseills, France). An intraoral X-ray machine (Biomedicare, Thane, India) was used to take the radiographs set at 65 kVp, 10 mA, 0.45-0.55 seconds. The sensor beam alignment aiming device was not used as it was difficult for many patients, especially pediatric patients, to hold the assembly in position. We present the cases where we used the extraoral technique to perform diagnostic imaging of patients who could not tolerate intraoral film placement.
Results
Case 1. Application in patient with mouth opening limitation
A 35-year-old male reported to our department with complaints of pain and swelling in maxillary left posterior region. On clinical examination, patient had masseteric space abscess secondary to caries on the maxillary left first and second molars. Patient also had a restricted mouth opening of 25 mm. In this patient, radiographs were obtained using both the conventional intraoral periapical radiographic technique and extraoral periapical technique. Figure 2 shows the comparison between standard intraoral periapical radiograph (A) and radiograph using extraoral technique (B). As seen, the radiograph obtained by extraoral technique has an adequate diagnostic value. Patient found the extraoral technique less painful and comfortable.
Case 2. Application in endodontics
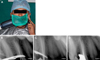
A 34-year-old male patient reported to our department with complaints of dull and aching pain in the upper left posterior region. Intraoral examination revealed a deep occlusal caries associated with the left maxillary second premolar. The tooth was tender on percussion. The patient had a severe gag reflex and it was impossible to obtain conventional intraoral periapical radiograph. A provisional diagnosis of apical periodontitis was made and endodontic treatment was recommended. The caries was excavated and adequate access cavity was prepared. Two root canals were located. However, it was impossible to obtain a radiograph to measure the working length. Therefore, it was decided to perform the extraoral periapical radiographic technique. The patient was positioned upright, with her mouth open as wide as possible. The sensor was placed on the external surface of the cheek, directly buccal to the left maxillary second premolar. A cotton roll was placed between the sensor and the cheek to parallel the sensor with the buccal surface of the tooth. The X-ray cone was angled approximately -25 degrees from the horizontal plane (Fig. 3A). The radiograph was taken with #15 K files (Fig. 3B). Cleaning and shaping of the root canals were performed and a radiograph with a master cone was obtained. The post-operative radiograph was obtained after obturation in similar way which provided the adequate diagnostic details (Figs. 3C and D). The added advantage of this technique was that it could be used in the patients with rubber dam in place making it applicable for all phases in endodontic therapy.
Case 3. Application in pediatric patients
Pediatric patients are generally reluctant to intraoral film placement. A 7-year-old male patient reported with a complaint of severe pain in maxillary deciduous second molar region. On clinical examination the deciduous maxillary second molar was grossly carious. The patient was highly reluctant to intraoral placement of the sensor. Hence it was decided to use the extraoral technique. The technique for pediatric patients differed from that for adults. In pediatric patients we used lesser angulations i.e. -20 degrees for taking the radiographs of maxillary teeth and -10 degrees for taking the radiographs of mandibular teeth. The exposure time used over here was 0.35-0.40 second (Fig. 4A). The radiograph provided the essential diagnostic details (Fig. 4B) of the deep carious lesion extending into bifurcation, and it was decided to extract the tooth followed by placement of a space maintainer. Similarly, this technique was used in other non-cooperative pediatric patients (Figs. 4C and D). The patients found this technique less traumatic, and it was easier to obtain the patient cooperation.
Case 4. Application in oral surgery
Obtaining good intraoral radiographs of impacted third molar is often complicated by inadequate patient compliance and exaggerated gag reflex. Here we used this technique to obtain radiographs of impacted third molars in various patients. The technique used here was similar to the above mentioned technique. However, the sensor was placed more posteriorly and directly buccal to the third molars. The angulation used was -25 degrees for maxillary teeth and -10 degrees was used for mandibular teeth (Fig. 5A). The radiographs provided the essential diagnostic information (Figs. 5B and C). The patients preferred this technique compared with the conventional intraoral technique.
Discussion
Even though conventional intraoral radiography has been used widely in dental field, sometimes there are problems in taking the radiographs in pediatric patients, disabled patients, obtaining third molar radiographs, and obtaining radiographs in endodontics.1 In 1974, Fisher proposed an extraoral radiographic technique for obtaining images of third molars using occlusal films, however the requisite high kVp (as high as 90 kVp) had limitations in its daily clinical application.5 We found that, using a digital imaging system at 65 kVp, it was sufficient to produce the image with adequate diagnostic quality comparable with the conventional intraoral periapical radiographs.
This radiographic technique is not intended as a substitute for conventional intraoral radiography. According to Newman and Friedman,3 the angulation of -55 degrees for maxillary teeth and -35 for mandibular teeth was used. Chen et al4 advocated the use of lesser angulation than that given by Newmann and Friedman (-20° to -30° for maxillary teeth; -10° to -15° for mandibular teeth with reference to the horizontal plane). We used the angulation of -25 degree for maxillary and -15 degrees for mandibular teeth. However, the angulation can be changed according to the racial differences in facial height.
In our study we used the angulations of -20 degrees for maxillary teeth and -10 degrees for mandibular teeth respectively for pediatric patients due to the lower facial heights and the angulations of -25 degrees and -10 degrees for maxillary and mandibular teeth respectively to take the radiographs of impacted third molars.
It is a useful alternative technique and has proved to be effective in patients who are unable to tolerate the conventional technique. This technique might be used for the developmentally disabled patients, patients with exaggerated gag reflex, pediatric patients, dental phobic patients, trauma patients, patients with trismus, and so on.1,3,4 The advantage of this technique is the increased patient compliance providing images with adequate details and diagnostic quality.3,4 However, the disadvantages of this technique are the procedure being technique sensitive, slightly lower resolution of images, and inability to obtain radiographs of anterior teeth.3
With recent advances in dental radiology, various techniques like panoramic radiography are available to manage those patients, however this technique can be recommended in the dental clinics without panoramic radiographic machines.
In conclusion, this technique is not meant for replacing conventional intraoral radiography, however it can be used for replacing intraoral periapical radiography when intraoral film is difficult to place in patient's mouth. We recommend further standardization of this technique for superior image quality.




 XML Download
XML Download