

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Impaction of a tooth is a situation in which an unerupted tooth is wedged against another tooth (or teeth) or otherwise located so that it cannot erupt normally.1 The mandibular third molar is the most frequently impacted. Impacted mandibular third molars are categorized according to the anterior-posterior space between the second molar and the mandibular ramus, its medial-lateral position in the body of the mandible, and the position of its long axis. Ectopic mandibular third molars, however, are rare and usually found because of the clinical symptoms. Their heterotopic positions were reported to be in the condylar area, in the ascending ramus of the mandible, or in the coronoid process.2 Unilateral or bilateral ectopic impacted third molar teeth have been reported in various parts of the mandibular ramus.
This report presents an ectopic mandibular third molar in the mandibular condyle without any pathologic condition.
Case Report
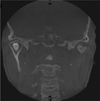
A 70-years-old woman visited the department with a complaint of discomfort on the left preauricular area during mastication and mouth opening, which had occurred 3 or 4 months before. On the clinical examination there was tenderness on the left preauricular area without any specific findings. Panoramic radiograph showed generalized alveolar bone destruction and calculus deposition. All the teeth showed moderate attrition. Additionally, a well-formed, impacted tooth was found in the right condylar head of the mandible. The tooth crown seemed to direct into the head of the condyle (Fig. 1).
The patient had no experience of extraction of third molars, and any associated pathologic sign was not observed. According to the orientation and location of the impacted tooth, it was considered as an ectopic impaction of a mandibular third molar.
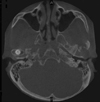
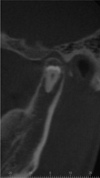
Cone beam CT scans were performed to evaluate the position and direction of the impacted tooth in the mandibular condyle. Coronal image showed the upward crown position of the impacted tooth (Fig. 2). There was no pathologic sign such as cystic change around the impacted tooth. On the axial image, an impacted tooth was found in close proximity to the front cortical bone and in the middle portion of the mandibular condyle (Fig. 3). Sagittal image showed a well developed impacted tooth with proximity to the outer cortical bone of the mandibular condyle (Fig. 4). The follicular space and lamina dura of the tooth were not distinguished. On the frontal view of 3D volumetric image, the crown of the impacted tooth was partially covered with bone (Fig. 5).
The mandibular condyle was not expanded. There was no pathologic or morphologic change on the surrounding bone. Final diagnosis was an ectopic impaction of the mandibular third molar in the mandibular condyle.
Discussion
The true incidence and etiology of ectopic impaction of mandibular third molar remain unknown. Several theories have been suggested to explain the ectopic eruption, including aberrant eruption, trauma, and ectopic formation of the germs of the teeth.2 It has been suggested that an aberrant eruption pattern occurred when the tooth has been displaced by a lesion, usually an odontogenic cyst.3
Wang et al3 in 2008 reported a similar case and reviewed the literatures from 1978 to 2003. They found 13 case reports of the ectopic third molars in the subcondylar area, including 1 case of a dry skull and 1 of a cadaveric mandible. The management for these conditions was described as no treatment or as surgical removal via extraoral or intraoral access. Salmerón et al2 in 2008 reported 2 cases of third molars in the subcondylar area, which were associated with odontogenic cysts and treated through the extraoral approach, indicating that the treatment was primarily determined by the experience of the surgeon or physician.
Wang et al3 reviewed that eight of the 11 cases included the description of a radiolucent image around the ectopic molar on the radiograph, including 5 with the diagnosis of a dentigerous cyst. These mandibular third molars might be displaced by the lesion. The expansion of a cyst might put pressure on the crown of a tooth and displace it in the opposite direction to the path of eruption. Several teeth had an upward whereas the others had a downward inclination or even an inverted crown position. In this case, the abnormal position of the tooth germ might be the most likely causative factor because the impacted tooth was positioned in the mandibular condyle with an upward crown position without any pathologic change which resulted in such unusual movement.
The surgical removal of an ectopic mandibular third molar with acute inflammation or cystic lesion is recommended to prevent further complications such as diffuse osteolysis, condylar process deformity, or bone absorption.4,5 In cases of symptom-free highly aberrant wisdom teeth or without urgent necessity, annual follow-up visits to monitor the growth of the lesion is appropriate.6,7 In this case, the impacted tooth was not removed because of the absence of the associated symptom or lesion unlike other reports2,4-6 and the patient's age.


 XML Download
XML Download