

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There has been an exceptional growth in the use of testosterone therapy (TTh) in the last decade [1]. This increase in usage has been attributed to many factors including age, poor general health and medical conditions such as obesity and diabetes [1]. It is known that testosterone (T) levels start to decline by an average of 3.1 to 3.5 ng/dL per year in men starting at age 30 [23]. Studies have estimated that there are approximately 2.4 million men in the US with testosterone deficiency (TD) between the ages of 40 and 69 years old [34], and this prevalence might increase to 6.5 million by 2025 in males with age between 30 and 80 [5].
Late-onset hypogonadism (LOH), also known as age-associated (TD), is a clinical and biochemical syndrome associated with increasing age and characterized by a set of signs and symptoms in combination with low serum T [678]. Symptoms include decreased libido, erectile dysfunction, decreased muscle mass and strength, increased body fat, decreased bone mineral density and osteoporosis, and decreased vitality and depressed mood [7]. The diagnosis of LOH can be challenging given that signs and symptoms are nonspecific and serum T levels do not appear to correlate directly with symptoms in all patients [17].
There has been an emerging controversy in the past several years regarding the safety of TTh due to a suggested increased risk of cardiovascular (CV) disease among its users. In 2015, the United States Food and Drug Administration (FDA) stated that TTh is only approved for congenital hypogonadism or acquired damage to the brain, pituitary gland, or testes, and not for age-related or comorbidity-associated LOH [9]. Nevertheless, only a minority of patients with LOH fulfill the criteria stated by the FDA, whereas the large majority of patients with TD present with comorbidities including obesity, metabolic syndrome and diabetes [1011]. The FDA statement extended their update secondary to two previous studies that reported a possible increased risk of heart attacks and strokes in patients taking TTh [1213]. These articles led to nation wide media coverage raising concerns that the pharmaceutical companies were promoting and “overselling” treatments that were “dangerous” and associated with important CV risks [14]. Furthermore, the FDA issued statements regarding CV safety of TTh products [15]. Although a thorough analysis of these studies was performed by several investigators as well as the FDA, all arriving at the conclusion that these studies were seriously flawed, the FDA mentioned in their statement that there is a possible increased CV risk associated with T use [9]. Given the growing prevalence of TD in our population and the increase use of TTh, the goal of this review is to present the history and emerging evidence in regards to the controversy surrounding TTh and CV risk.
Go to : 
HISTORY
1. Testosterone therapy and its association to cardiovascular events
TTh has been in the market for more than 70 years for the treatment of TD [16]. Early studies in the 1940s documented little risk and even reported benefits for peripheral vascular disease and angina pectoris [1517181920]. Lesser studied 100 patients (92 men and 8 women) from ages 34 to 77 with angina pectoris who received T propionate with a follow-up ranging from several months to 5 years. He noted improvement of angina pectoris in 91% of patients [19].
An abundance of studies in the last 20 years have published data that TD is associated with an increased risk of developing atherosclerosis, CV disease, worsening osteoporosis and increased mortality. Even more, TTh has been found to have a beneficial effect on multiple risk factors and biomarkers related to these conditions. Moskovic et al [21] attempted to quantify the cost burden imposed by TD's cardiometabolic sequelae. They projected that low serum T levels is involved in the development of approximately 1.3 million new cases of CV disease, 1.1 million new cases of diabetes, and over 600,000 of osteoporosis-related fractures. They also determined that, over a 20-year period, TD may be directly responsible for approximately $190 to $525 billion in inflation-adjusted US health care expenditures [21].
Considering diabetes, dyslipidemia, hypertension, and obesity are risk factors for CV disease, and that TD contributes to increased fat mass and insulin resistance, it is reasonable to believe that TD increases CV disease by potentiating these risk factors. Furthermore, any therapeutic modality that mitigates these risk factors is expected to reduce the risk of developing CV disease. Numerous intervention studies with the use of TTh demonstrate improvements in lipid profile, inflammation, obesity, waist circumference, glycemic control and blood pressure [15]. These findings have found a legitimate biological mechanism to explain the increased mortality among men with TD [15222324].
2. Clinical trials reporting increased cardiovascular risk
The first trial we found reporting adverse CV effects after TTh was the Testosterone in Older Men with Mobility Limitations (TOM) trial by Basaria et al [25] in the New England Journal of Medicine. This was a prospective, placebo-controlled, randomized trial that was designed to determine the effects of 6 months of TTh on lower-extremity strength and physical function in older men (n=209) with TD and limited mobility. They found a benefit for functional status and muscular strength response but the trial was terminated early because of increased CV adverse effects in the treatment group (21.6% vs. 4.8% in placebo group). Nevertheless, of the 23 reported CV events, only four were considered major adverse cardiac events (MACE). Morgentaler et al [15] pointed out in their analysis of this study that “this asymmetry is not uncommon with rare events in clinical trials”; and, this was demonstrated by a similar study earlier that year which reported 2 MACE events, both of which occurred in the placebo group [26]. Moreover, this study was not designed or powered to investigate CV events, and these “events” were not primary or secondary end points but only found incidentally and some considered of questionable clinical importance such as pedal edema and palpitations. The authors even concluded that the CV adverse events reported in their trial warrant “caution in interpretation” since “The lack of a consistent pattern in these events and the small number of overall events suggest the possibility that the differences detected between the two trial groups may have been due to chance alone” [25].
In early 2014, two published articles had gained media attention after they reported that patients who received TTh were at an increased risk of developing CV disease [1213]. Vigen et al [12] published a retrospective national cohort study of 8,709 men with a total T level lower than 300 ng/dL who had undergone coronary angiography within the Veterans Administration (VA) health care system. They aimed to evaluate the association between the use of TTh and all-cause mortality, myocardial infarction (MI), and stroke. Study group consisted of 1,223 patients compared to 7,486 controls and the average follow-up was 27.5 months overall. TTh treatment was defined as filling a single prescription for any T product. Therefore, this definition cannot be extrapolated to the use of long-term TTh. Even though there were no statistically significant differences in overall rate of events at 180, 365, and 540 days, the authors reported that the overall rate of MI, stroke and death was higher in men receiving TTh when compared to untreated men. However, the actual rate of adverse events was half (10.1%) in the treatment group vs. 21.2% in the control group. The authors failed to acknowledge these numbers and came to a paradoxical interpretation based on complex statistics that included adjustment for more than 50 variables [15]. Moreover, after multiple criticisms, the article underwent 2 official corrections, one for misreporting primary results as “absolute risk” which suggested results were based on raw data which led to the term correction of ‘Kaplan-Meier estimated cumulative percentages with events’, which highlights the highly statistical nature of the published results [27]. The second correction came 2 months later in response to a letter that challenged the exclusion of men who had suffered adverse events in the non-T group. The number was changed from 1,132 to 128 men [28]. More remarkable was the fact that they initially included 100 women in the all-male study group. All these errors prompted many medical societies and physicians from multiple countries to request a retraction of this article [29].
The second article that gained media attention was published by Finkle et al [13] in early 2014. It was a retrospective cohort study from a health insurance database that reported a comparison of rates of nonfatal MI in the period up to 90 days after T prescription vs. MI rates 12 months prior to T prescription. The database included a total of 55,593 subjects with a post-prescription period defined as time to first prescription refill, which ranged from 30 to 90 days. Patients who did not refill their initial prescription were analyzed an additional 90 days (total of 180 days). These patients were compared to a control group which consisted of 167,279 men who received a prescription for a phosphodiesterase type 5 inhibitor (PDE5i). Authors found an increased relative risk (RR) of 1.36 of MI post-T prescription to pre-prescription. This was even higher in a subgroup analysis of men older than 65 years old (RR, 2.19). They reported no increase in MI rate (RR, 1.15) in the PDE5i group. However, the study had several flaws. First of all, the endpoint in the study, nonfatal MI, was determined by use of an insurance diagnosis code without medical record verification that an MI actually occurred. An error rate as high as 12% has been reported in previous studies when such measures are not clarified [1530]. Moreover, comorbidities and CV risk factors such as diabetes, hypertension, smoking history, and elevated cholesterol were not accounted for. Furthermore, they compared the treatment group with men who received PDE5is, a medication that is used for a different indication, making the comparison dissimilar and unparalleled. It is unknown whether the prescriptions were ever filled and even if they were, a short and limited exposure to TTh of 30 to 90 days allows for the possibility that any observed increased risk of MI was secondary to an underlying condition rather than from TTh. The FDA concluded in July 2014 that “it is difficult to attribute the increased risk for non-fatal MI seen in the Finkle study to T alone and not consider that the study participants might have remained hypogonadic and thus at higher risk for non-fatal MI” [31].
The CV events reported in these trials studying the effects of TTh have been diverse, suggesting that more than one mechanism might be responsible. Some animal studies have shown that TTh up-regulates the renin- angiotensin system and therefore, promotes sodium reabsorption in the kidneys which in turn could lead to fluid retention and hypertension [3233]. Some have suggested that TTh induces aggregability of platelets by increasing thromboxane A2 receptor density on human platelets which may increase hypercoagulability and thrombosis [34]. Moreover, erythrocytosis resulting from T administration may increase blood viscosity, create shear stress on the endothelial wall and eventually trigger plaque destabilization and rupture [35363738]. An overview of clinical studies reporting increased CV risk are summarized in Table 1.
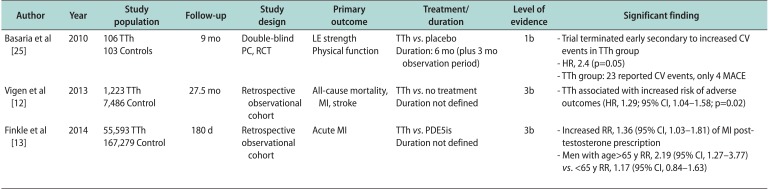
Table 1
Summary of clinical trials reporting increased CV risk after TTh
| Author | Year | Study population | Follow-up | Study design | Primary outcome | Treatment/duration | Level of evidence | Significant finding |
|---|---|---|---|---|---|---|---|---|
| Basaria et al [25] | 2010 |
106 TTh 103 Controls |
9 mo |
Double-blind PC, RCT |
LE strength Physical function |
TTh vs. placebo Duration: 6 mo (plus 3 mo observation period) |
1b | - Trial terminated early secondary to increased CV events in TTh group |
| - HR, 2.4 (p=0.05) | ||||||||
| - TTh group: 23 reported CV events, only 4 MACE | ||||||||
| Vigen et al [12] | 2013 |
1,223 TTh 7,486 Control |
27.5 mo | Retrospective observational cohort | All-cause mortality, MI, stroke |
TTh vs. no treatment Duration not defined |
3b | - TTh associated with increased risk of adverse outcomes (HR, 1.29; 95% CI, 1.04–1.58; p=0.02) |
| Finkle et al [13] | 2014 |
55,593 TTh 167,279 Control |
180 d | Retrospective observational cohort | Acute MI |
TTh vs. PDE5is Duration not defined |
3b | - Increased RR, 1.36 (95% CI, 1.03–1.81) of MI post-testosterone prescription |
| - Men with age>65 y RR, 2.19 (95% CI, 1.27–3.77) vs. <65 y RR, 1.17 (95% CI, 0.84–1.63) |
![]()
Go to :
EMERGING EVIDENCE
1. Clinical trials reporting cardiovascular events
The TTrials were a group of 7 randomized placebo-controlled trials that were designed to determine the efficacy of TTh on men aged 65 years or older with low serum T levels [39]. TD was verified by serum levels of <275 ng/dL on 2 different lab draws. A total of 790 men were randomized to apply topical T gel vs. placebo for 12 months. Although CV events were not a primary end point, adverse CV events were recorded at every 3-month visit and a CV-event questionnaire was administered. They found no difference in the number of CV events between groups with seven men in each group adjudicated to have a MACE during the 1-year treatment period (Table 2).
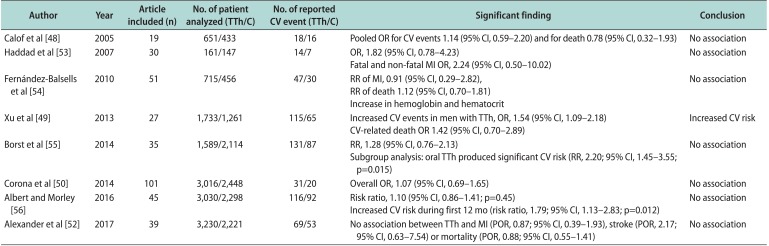
Table 2
Summary of clinical trials reporting no association between TTh and CV risk
| Author | Year | Study population | Follow-up | Study design | Primary outcome | Treatment/duration | Level of evidence | Significant finding |
|---|---|---|---|---|---|---|---|---|
| Wallis et al [41] | 2016 |
10,311 TTh 28,029 Controls |
5.3 y | Retrospective, observational cohort | Overall mortality, (secondary=CV outcomes) |
TTh vs. no TTh Duration: median 2–35 mo |
3b | - Cumulative mortality lower in TTh vs. controls (p<0.0001) |
| - No difference in CV events between groups (p=0.25) at 5 y | ||||||||
| - Short duration of TTh associated with increased mortality (p<0.0001) and CV risk (p=0.0002) | ||||||||
| Snyder et al [39] | 2016 |
394 TTh 394 Controls |
24 mo | Double-blind, PC, RCT | Sexual function, physical function and vitality |
TTh vs. placebo Duration: 12 mo |
1b | - Significant change from baseline in TTh group on all primary outcomes (p=0.006) |
| - MACE: 2 in TTh, 9 in placebo | ||||||||
| - No association between TTh and CV risk | ||||||||
| Anderson et al [42] | 2016 |
801 Low T 2,241 Normal T 1,694 High T |
3 y | Retrospective, observational cohort | MACE as a composite of death, nonfatal MI, and stroke | TTh at 1 and 3 y | 3b | - Normalized T group had reduced MACE (p=0.04) and CV related death (p=0.009) |
| - High T group showed trend to increased stroke risk, but not statistical difference (p=0.16) | ||||||||
| Maggi et al [43] | 2016 |
750 TTh 249 Controls |
3 y | Prospective, observational cohort | Prostate health outcomes and CV safety |
TTh vs. no TTh Duration: 3 y |
2b | - CV rate not statistically different between groups (p=0.7) |
| Budoff et al [40] | 2017 |
73 TTh 65 Controls |
24 mo | Double-blind, PC, RCT | Noncalcified CAPV |
TTh vs. placebo Duration: 12 mo |
1b | - TTh associated with a significant greater increase in noncalcified CAPV (p=0.003) |
| - MACE: none reported in either group | ||||||||
| Traish et al [44] | 2017 |
360 TTh 296 Controls |
8 y | Prospective observational cohort | Mpsa |
TTh vs. no TTh Duration: not defined |
2b | - Increased number of deaths secondary to CV disease, nonfatal MIs and strokes in control group. |
| - TTh had significant reduction in all Mpsa | ||||||||
| Sharma et al [45] | 2017 |
- 40,856 TTh with normal T level - 23,939 TTh with nonnormal T - 11,853 No TTh |
6 y (mean) | Retrospective observational cohort | Afib |
TTh vs. no TTh Duration: not defined |
3b | - Decreased Afib risk in the normalized TTh group vs. nonnormalized TTh group (p=0.0255), and untreated group (p=0.0001) |
TTh: testosterone therapy, CV: cardiovascular, T: testosterone, PC: placebo-controlled, RCT: randomized controlled trial, MACE: major adverse cardiac event, MI: myocardial infarction, CAPV: coronary artery plaque volume, MPs: multiple parameters, Afib: atrial fibrillation.
aWeight, waist circumference, body mass index, hemoglobin A1c, systolic and diastolic blood pressure, heart rate, lipid profile, C-reactive protein, and liver transaminases.
![]()
Budoff et al [40] conducted the CV Trial, which was part of the TTrials, and used computed tomography angiography scan to assess if TTh slows the progression of noncalcified coronary artery plaque volume as an indicator of coronary atherosclerosis. Of 170 enrolled men, 138 patients with a mean age of 71.2 years completed the study. They reported that the TTh group was associated with a significantly greater increase in noncalcified plaque volume after 12 months of treatment when compared with placebo (p=0.003). However, there were no MACE events reported in either group. Even though these findings are hard to extrapolate to general practice given the small cohort and short follow-up, they imply that thrombosis of this growing coronary plaque may explain some of the CV events previously reported that occur early after initiation of TTh [4142].
Anderson et al [42] performed an observational-retrospective analysis that assessed the safety and CV outcomes of TTh in a study cohort of 4,736 men with a diagnosis of TD (confirmed with T level of <212 ng/dL) after 1 and 3 years of TTh. On follow-up T testing, they divided the subjects into 3 groups: low (<212 ng/dL), normal (212–742 ng/dL), and high (>742 ng/dL) T levels. Average age among groups was 61.2 years. Overall, 3 year rates of MACE and death were reported as 6.6% and 4.3%, respectively. Multivariate adjusted hazard ratio (HR) revealed that patients who had TTh and reached normal T levels had reduced MACE (HR, 0.74; p=0.04) and CV-related death (HR, 0.65; p=0.009) at 3 years compared to low T. Patients with high T levels had no significant risk of MACE at 3 years when compared to low T. Although the risks of MI and stroke were low over 3 years, the adjusted HR trended to a higher stroke rate on patients with high T when compared to low and normal T (HR, 1.69 and 1.53, respectively; p=0.16). The mechanisms contributing to lower mortality while increasing stroke risk are uncertain and require further investigation.
The Registry of Hypogonadism in Men (RHYME) was a multi-national, prospective cohort of men with LOH designed to evaluate both prostate health outcomes and CV safety [43]. Although the study was not originally powered to determine differences in mortality or CV events between men treated with TTh compared with untreated men, they were able to document CV event rates during their 36-month follow-up. They analyzed 999 men of which 750 were in the TTh group. No overall associations were observed between the 55 reported adverse CV events and overall TTh use or duration. There was no statistically significant difference in overall incidence rates for CV events between groups (p=0.7), even when the analysis was stratified for age. Adverse CV events rates were significantly related to age (p≤0.0001), body mass index (BMI) (p=0.05), smoking (p=0.03), and comorbidities (p=0.01), but not to TTh use (p=0.68). Limitations in this study included lack of randomization, and absence of recorded data on the rationale for patient or physician choice for receiving TTh and type of TTh selected. Moreover, there was variability in the degree of serum T normalization with treatment. Nevertheless, this contributes to the major strength of this study which is the simulation to what physicians may encounter in the real world. The authors of this study plan to obtain 10-year follow-up date which may aid to investigate the long-term effects of TTh.
The most recent study we found was an observational, prospective, cumulative registry study that attempted to assess the long-term effectiveness of TTh in 645 men with diagnosed LOH, of which 360 received parenteral T and 296 men opted to receive no treatment [44]. Median follow-up was 7 years. To account for baseline differences between the 2 groups, changes were adjusted for age, weight, waist circumference, fasting glucose, blood pressure and lipids. The study reported 2 deaths non-related to CV events in the TTh group vs. 21 deaths in the control group of which 19 were related to CV events. They also noted 26 nonfatal MIs and 30 nonfatal strokes in the control group and none in the TTh group. After adjustment for baseline differences, they reported that men receiving TTh had a significant reduction in blood glucose (p<0.0001), systolic (p<0.0001) and diastolic (p<0.0005) blood pressure, liver enzymes (p<0.0001), lipid profiles (p<0.0001), weight (p<0.0001), waist circumference (p<0.0001) and BMI (p<0.0005). Conversely, patients in the control group showed no change or worsening of these parameters at the 8-year analysis. A major limitation of this study was the fact that patients who served as controls were those who, primarily due to financial reasons, opted against TTh. Socioeconomic status is known to have an influence in overall health and CV health. For this reason, it is possible that the unfavorable outcomes noted in the control group were secondary to a lower income and therefore, overall poor health.
We were able to find only one study that assessed the effect of duration of TTh exposure on mortality and CV events. Wallis et al [41] conducted a retrospective population-based matched cohort study of men 66 years or older newly treated with TTh (n=10,311) vs. controls (n=28,029) matched to age, region of residence, and comorbidities such as diabetes. Median follow-up was 5.3 years in the treatment group vs. 5.1 years in the control group. Primary outcome was overall mortality with secondary outcomes included composite CV outcomes (MI, stroke, or venous thromboembolic event) and prostate cancer diagnosis. Median time to CV event was not found to be statistically significant (p=0.95) between groups (30.4 months and 30.9 months in treatment vs. control groups, respectively). They reported an inverse association between cumulative TTh and mortality/CV events. Short durations of therapy (median 2 months) were associated with an increased risk of mortality and CV events, whereas a median duration of 35 months of TTh was associated with reduced mortality and CV events when compared to controls. Given this was a survival analysis, limitations included the fact that they only considered the first event for each patient for each outcome. Hence, any event that occurred after the first reported event was not included in the analysis. Furthermore, they did not compare patients with LOH since their database did not document presence of TD which itself questions the adequacy of therapy in these patients. They concluded that there results “should be considered hypothesisgenerating rather than definitive” and should be further validated in a prospective randomized setting.
2. Clinical trials reporting arrhythmias
There are few studies that have investigated the effect of TTh on arrhythmias. Sharma et al [45] studied whether normalization of serum T levels after TTh has an impact on the incidence of atrial fibrillation (Afib). They retrospectively compared patients at the US VA who received TTh and resulted in normalization of serum T (n=40,856), patients who received TTh without normalization of serum T (n=23,930), and those who did not receive TTh and continued to have low serum T (n=11,853). Mean follow-up was 6 years for the normalized TTh group, 4.4 years for non-normalized TTh group, and 4.5 years for the untreated group. Inverse probability weighting was used to analyze the different groups and remove the result of confounding when estimating the effect of treatment on outcomes. The study showed a significant lower risk of AFib in the normalized TTh group when compared to the nonnormalized TTh group (HR, 0.90; 95% confidence interval [CI], 0.81–0.99; p=0.0255) and untreated group (HR, 0.79; 95% CI, 0.70–0.89; p=0.0001). They also found no statistically significant decrease in Afib-risk between the non-normalized TTh group and untreated group (HR, 0.89; 95% CI, 0.78–1.009; p=0.0675). Given that the cohort was obtained from a large number of different VA hospitals, there was wide variability in the units used to express T test result. Therefore, instead of using a discrete cutoff value for what was considered low T, they considered low T according to the lower limit of the normal reference range of each laboratory, which could have confounded results.
Sharma et al [45] highlighted that normalization of T levels is associated with a lower incidence of Afib in men with LOH. Although the mechanism by which normal T levels reduce the risk of Afib is still unclear, their study suggested that TTh may have antiarrhythmogenic properties. This hypothesis has been supported by other studies that have demonstrated an association between low T and an increased risk of Afib [4647]. Nevertheless, the strength of the association between LOH and Afib needs to be further assessed and compared with the strength of other established risk factors. Interestingly, these findings were not supported by other trials discussed in this review such as the TOM trial, which found 3 Afib episodes in the TTh group compared with none in the placebo [25], and the TTrials which reported 11 hospitalizations for arrhythmias in the T group compared to only 7 in the placebo group [39].
3. Meta-analyses reporting cardiovascular events
Several systematic reviews and meta-analyses have pooled data from randomized controlled trials (RCTs) to examine the association between exogenous T and CV health with conflicting results [484950515253545556]. Onasanya et al [51] published an overview of systematic reviews and meta-analysis that studied the association between TTh and CV events. Six out of seven systematic reviews showed no association between exogenous T and CV events [485053545556], although two of these 6 studies showed increased risk in subgroup analyses of oral T and men aged 65 years or older during their first year of treatment [5556]. The systematic review that showed an association was published by Xu et al [49], who reported more CV events in men who received TTh (OR, 1.54; 95% CI, 1.09–2.18) compared to those who received placebo. Among the 2,994 men in their 27 trials reviewed, there were a total of 180 reported CV-related events, of which 115 were in the TTh group. Interestingly, they included 2 studies that require a closer examination. The first one was a trial conducted by The Copenhagen Study Group for Liver Diseases [57] who used an extremely high dose (600 mg/d) of micronized T in men who had a known diagnosis of liver cirrhosis, which resulted in exceedingly high concentrations of serum T and worsening of their disease. Moreover, they catalogued any bleeding event as CV, which with their history of cirrhosis, most events were secondary to hepatic complications such as bleeding from esophageal varices. Copenhagen reported only 1 MI out of the 21 listed CV events. The second study was the TOM trial by Basaria et al [25] which we previously mentioned. Taking into consideration that Basaria et al [25] had 4 (out of 23) MACE events, inclusion of all other CV events altered the final results of this meta-analysis.
The most recent meta-analysis found was reported by Alexander et al [52], who in contrast to previous systematic reviews, used meta-analytic techniques (e.g., Peto odds ratio [POR]) that were appropriate for rare events and examined the risks of events such as MI and/or stroke separately rather than as an aggregate outcome representing all CV events. They included 39 RCTs and 10 observational studies in their review. Follow-up in RCTs ranged from 6 weeks to 3 years. Primary outcomes were death, MI, and stroke. The 39 RCTs included 5,451 men of whom 3,230 were randomized to receive TTh and 2,221 placebo. MI was reported in 17 RCTs, stroke in 9, and mortality due to any cause in 21 trials. There were 16 trials included in the meta-analysis for MI, 9 trials for stroke, and 20 for all-cause mortality. Their findings showed no association between TTh and MI (POR, 0.87; 95% CI, 0.39–1.93), stroke (POR, 2.17; 95% CI, 0.63–7.54), or mortality (POR, 0.88; 95% CI, 0.55–1.41). A total of 30 trials were included in the quantitative synthesis on the composite outcome of death, MI, and stroke and this showed no statistically significant increased risk (POR, 0.96; 95% CI, 0.65–1.42). Limitations of this study were mostly represented by limitations in the individual studies such as failure to report detailed reasons for study withdrawal, short follow-up or duration, possibility of publication bias with respect of reporting potential harms, and the inability to use patient level data in their analysis which is common to happen in meta-analyses and systemic reviews. The strength of this review was the use of a meta-analytic approach that is robust for sparse data (Table 3).
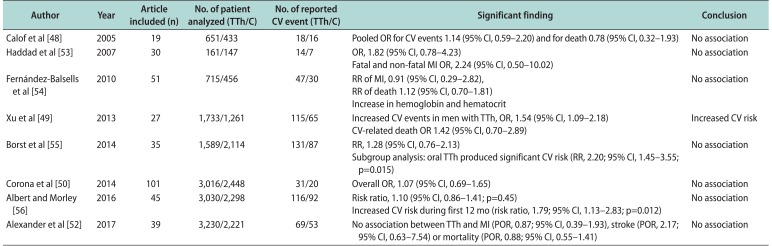
Table 3
Meta-analyses reporting CV risk with TTh
| Author | Year | Article included (n) | No. of patient analyzed (TTh/C) | No. of reported CV event (TTh/C) | Significant finding | Conclusion |
|---|---|---|---|---|---|---|
| Calof et al [48] | 2005 | 19 | 651/433 | 18/16 | Pooled OR for CV events 1.14 (95% CI, 0.59–2.20) and for death 0.78 (95% CI, 0.32–1.93) | No association |
| Haddad et al [53] | 2007 | 30 | 161/147 | 14/7 | OR, 1.82 (95% CI, 0.78–4.23) | No association |
| Fatal and non-fatal MI OR, 2.24 (95% CI, 0.50–10.02) | ||||||
| Fernández-Balsells et al [54] | 2010 | 51 | 715/456 | 47/30 |
RR of MI, 0.91 (95% CI, 0.29–2.82), RR of death 1.12 (95% CI, 0.70–1.81) |
No association |
| Increase in hemoglobin and hematocrit | ||||||
| Xu et al [49] | 2013 | 27 | 1,733/1,261 | 115/65 | Increased CV events in men with TTh, OR, 1.54 (95% CI, 1.09–2.18) | Increased CV risk |
| CV-related death OR 1.42 (95% CI, 0.70–2.89) | ||||||
| Borst et al [55] | 2014 | 35 | 1,589/2,114 | 131/87 | RR, 1.28 (95% CI, 0.76–2.13) | No association |
| Subgroup analysis: oral TTh produced significant CV risk (RR, 2.20; 95% CI, 1.45–3.55; p=0.015) | ||||||
| Corona et al [50] | 2014 | 101 | 3,016/2,448 | 31/20 | Overall OR, 1.07 (95% CI, 0.69–1.65) | No association |
| Albert and Morley [56] | 2016 | 45 | 3,030/2,298 | 116/92 | Risk ratio, 1.10 (95% CI, 0.86–1.41; p=0.45) | No association |
| Increased CV risk during first 12 mo (risk ratio, 1.79; 95% CI, 1.13–2.83; p=0.012) | ||||||
| Alexander et al [52] | 2017 | 39 | 3,230/2,221 | 69/53 | No association between TTh and MI (POR, 0.87; 95% CI, 0.39–1.93), stroke (POR, 2.17; 95% CI, 0.63–7.54) or mortality (POR, 0.88; 95% CI, 0.55–1.41) | No association |
![]()
It is known that in regards to all meta-analyses, results are greatly influenced by the definitions of end points of interest and selection of studies. Furthermore, in order to truly assess what happens in real-life settings, we would need randomized control trials with long durations approaching a decade. Given that most studies are of short duration, this is currently not feasible. In order to adequately power a clinical trial for rare outcomes, Onasanya et al [51] concluded in their optimal information size analysis that “any RCT aiming to detect a true difference in CV risk between treatment groups receiving exogenous T and their controls (with a two-sided p-value of 0.05 and a power of 80%) would require at least 17, 664 participants in each trial group”.
Go to :
CONCLUSIONS
Most patients who start TTh do so to find symptomatic relief from LOH and improve their quality of life. Some researchers have even suggested cycling TTh as an alternative option to continuous TTh to decrease the likelihood of adverse effects while still benefiting from LOH-related symptom relief [5859]. However, the overall benefit and safety of exogenous T has not been well established for age-related low T levels [9]. We included information from clinical trials and meta-analyses that assessed the relationship between TTh and CV risks. The FDA has required that pharmaceutical companies that produce TTh products do a trial to clarify and delineate the incidence of MACE in men with TD [51]. Unfortunately, the association between TTh and CV risk will continue to be debated for quite some time. Until this controversy is clarified, health-care professionals should continue to inform their patients about the possible CV risk when prescribing TTh products to their patients.
Go to :
 XML Download
XML Download