

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Priapism is a relatively uncommon condition that has been defined as a persistent erection unrelated to sexual stimulation, as well as a full or partial erection lasting more than four hours beyond sexual stimulation. The condition is aptly named after Priapus, the Greek god of fertility who was often depicted with a large phallus. The prolonged erection observed in priapism can be explained by disequilibrium between mechanisms regulating penile tumescence and flaccidity [1].
The incidence rate of priapism among males in the United States is 1.5 per 100,000 person-years [2]. When stratified for age, incidence rates peaked between the ages of 5 to 10 years and 20 to 50 years, with sickle cell disease being a common etiology due to mechanisms involving vaso-occlusion or decreased nitric oxide bioavailability [34]. Unfortunately, the incidence of priapism cannot be accurately reported because data from healthcare institutions only accounts for cases that seek medical care. As a result, such data are likely underestimating the true incidence of priapism in the male population.
There is a myriad of pharmacologic and surgical treatment modalities in the urologist's toolkit to manage priapism. While the subtype and etiology of priapism may dictate the use of different forms of management, the goals in treating all patients with priapism remains the same: to achieve detumescence, preserve erectile function, and reduce the risk of future episodes [1]. Unfortunately, given the low incidence of priapism and heterogeneity of clinical presentation, there is a considerable lack of randomized-controlled studies that measure the safety and efficacy of priapism therapies. This has made it difficult to develop strict evidence-based guidelines to direct clinicians. Fortunately, expert consensus supplemented with the most current literature provides a strong framework for physicians to manage priapism. Treatment options for priapism are often applied in a step-wise fashion, balancing the risks of invasive treatment against the consequences of prolonged cavernosal ischemia and permanent erectile dysfunction (ED) when treatment is delayed [5]. Regardless of the etiology, risk factors, or inciting event, the first goal of evaluation of priapism is distinguishing it as either ischemic or non-ischemic. This ensures effective and timely management of ischemic priapism, thereby reducing the likelihood of irreversible complications (i.e., ED, penile disfigurement, and gangrene).
Go to : 
DIAGNOSIS AND TREATMENT
1. Treatment of ischemic priapism
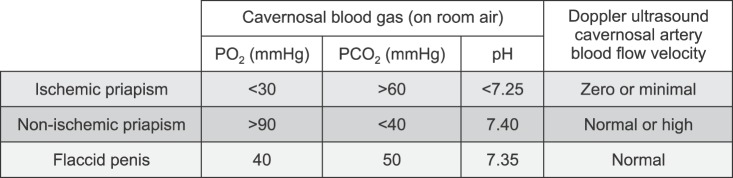
Ischemic, i.e., veno-occlusive or low-flow priapism, is the most common form of priapism and is characterized by persistent painful and fully rigid erections that last longer than four hours. It is estimated that 80% to 95% of cases of priapism meet ischemic criteria [67]. Ischemic priapism is considered a medical emergency and requires immediate intervention. Ischemic priapism is also associated with abnormal cavernosal blood gas values (hypercapnia, hypoxia, acidosis; Fig. 1), a characteristic that can assist in differentiating it from cases of high-flow priapism. Patients with congenital hematologic disorders (i.e., sickle cell disease), or hematologic malignancy preferentially experience ischemic priapism due to malfunctions in the detumescence pathway. Ischemic priapism is also associated with progression of fibrosis of the corpus cavernosa and development of ED. Studies have revealed that the longer the duration of untreated ischemic priapism, the higher the likelihood of ED [89].
The first-line treatment for ischemic priapism is therapeutic corporal aspiration with or without corporal irrigation [131011]. This involves insertion of an 18~19-gauge needle at the base of the penis in the 3 o'clock and/or 9 o'clock position, and aspiration of the blood using a syringe. To improve aspiration of stagnant blood within the corpora, sterile 0.9% saline may be used for irrigation. This practice is endorsed by the European Association of Urology, but not the American Urological Association (AUA), which has concluded there is no difference in resolution rates with or without irrigation [110]. Unfortunately, aspiration and irrigation alone have been shown to resolve ischemic priapism in only 36% of cases. If aspiration and irrigation fails to achieve detumescence, intracavernosal injection of sympathomimetics such as phenylephrine (alpha-1 adrenergic agonist) is indicated as second-line therapy. For healthy adults without cardiovascular comorbidities, 1.0 mL of 100 to 500 µg phenylephrine/mL of normal saline is injected into the corpora every 3 to 5 minutes until detumescence is achieved (Table 1) [1121314]. The combination of phenylephrine injection with corporal aspiration has demonstrated to resolve symptoms in 81% of patients. Injection of phenylephrine alone was only 58% effective. Thus, the effect of aspiration and sympathomimetic injection has additive efficacy. It is important to note that children and patients with pre-existing cardiovascular disease should receive a lower concentration and volume of phenylephrine. Alternatively, patients with cardiovascular disease may benefit from a transient distal penile corporoglanular shunt technique. This technique involves placement of a needle into the corpora cavernosa and another needle in the glans, which are then connected by external tubing to cause shunting of blood into the corpus spongiosum. Once detumescence is achieved, the needles and tubing are removed. This method was shown to resolve ischemic priapism within 10 minutes in 73.3% of patients, which was superior to phenylephrine alone (58%) and aspiration alone (36%), without the added cardiovascular risk of sympathomimetic therapy [11]. During injection of any vasoconstrictive agent, all patients should be monitored for hemodynamic instability due to the risk of hypertension, tachycardia, reflex bradycardia, and arrhythmias that can occur if phenylephrine leaks into the systemic circulation. Phenylephrine should be avoided in those taking monoamine oxidase inhibitors (i.e., isocarboxazid, phenelzine, selegiline, tranylcypromine) due to the risk of inducing a hypertensive crisis. If intracavernosal injections fail to provide improvement within one hour, the clinician needs to escalate the treatment through the creation of a surgical shunt [5].
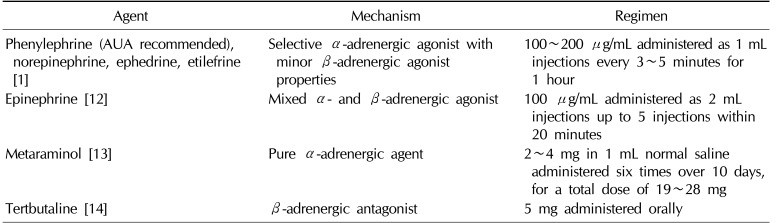
Table 1
Pharmacologic dosing for medical or intracavernosal treatment of ischemic priapism
| Agent | Mechanism | Regimen |
|---|---|---|
| Phenylephrine (AUA recommended), norepinephrine, ephedrine, etilefrine [1] | Selective α-adrenergic agonist with minor β-adrenergic agonist properties | 100~200 µg/mL administered as 1 mL injections every 3~5 minutes for 1 hour |
| Epinephrine [12] | Mixed α- and β-adrenergic agonist | 100 µg/mL administered as 2 mL injections up to 5 injections within 20 minutes |
| Metaraminol [13] | Pure α-adrenergic agent | 2~4 mg in 1 mL normal saline administered six times over 10 days, for a total dose of 19~28 mg |
| Tertbutaline [14] | β-adrenergic antagonist | 5 mg administered orally |
![]()
Surgical shunting involves creating an alternative pathway for hypoxic blood to exit the corpora. These shunts can be stratified into two main subtypes: distal or cavernoglandular shunts (Winter, Ebbehoj, T-shunt, Al-Ghorab) and proximal shunts (Quackels/corporal-spongiosum shunt, Grayhack/corporal-saphenous shunt) [110]. The less invasive forms of distal shunt (Winter, Ebbehoj, unilateral T-shunt) are initially attempted, given their lower risk of complication. Although proximal shunts have better efficacy in achieving detumescence, they also carry a greater risk of ED (50% with proximal vs. 25% or less with distal shunts) [15]. It should also be noted that less invasive distal shunts, such as the Winter shunt, can be performed in an emergency setting under local anesthesia, while more invasive shunts, such as the Al-Ghorab and proximal shunts, must be performed in an operating room under general anesthesia. Distal shunts involve inserting a biopsy needle (Winter) or scalpel (Ebbehoj) percutaneously to create a fistula between the corpora and the glans penis. More invasive distal shunts can also be performed by creating perpendicular scalpel cuts in the shape of a ‘T’ in the distal glans either uni- or bilaterally (T-shunt), or excising distal portions of the tunica albuginea to drain the corpora (Al-Ghorab). Studies have demonstrated a resolution rate of 66%, 73%, and 74% for Winter, Ebbehoj, and Al-Ghorab shunts, respectively [15]. The efficacy of the T-shunt and Al-Ghorab shunts can be improved to nearly 100% when combined with the use of dilators to physically remove stagnant blood within the corpora [161718]. However, use of dilators is accompanied by an increased risk of urethral injury and possible formation of urethrocavernosal fistulas [19]. Should distal shunts fail, the use of proximal shunts is warranted. The Quackels shunt creates a fistula between the corpora cavernosa and corpus spongiosum. In contrast, the Grayhack shunt utilizes an anastomosis between the corpora cavernosa and saphenous vein. Studies have demonstrated the efficacy of Quackels and Grayhack shunts to be equivalent (77% vs. 76%), and as such the AUA does not recommend one procedure over the other [1].
If shunting procedures fail, placement of a penile prosthesis (PP) may be considered, as the majority of patients with refractory priapism will experience fibrosis of the corpora and resultant ED. Indications and techniques for placement of a PP will be discussed in later sections of this review.
2. Treatment of stuttering priapism
Stuttering priapism is a chronic, recurrent form of ischemic priapism that occurs over many years and is often observed in patients with sickle cell disease. Patients with acute exacerbation of their stuttering priapism are treated in the same manner as patients with ischemic priapism. However, to reduce the risk of future episodes, adult patients may benefit from gonadotropin-releasing hormone antagonists or luteinizing hormone-releasing hormone agonists combined with antiandrogens. Intracavernosal injection of phenylephrine on demand may also be used for patients who cannot tolerate or afford hormonal therapy, ketoconazole, and phosphodiesterase-5 inhibitors [81720]. Therapies currently not recommended by the AUA include prostate massage, ice packs, and enemas, as well as oral agents such as terbutaline or pseudoephedrine [1].
3. Treatment of non-ischemic priapism
Non-ischemic or high-flow arterial priapism, is characterized by a non-painful erection lasting longer than four hours, that is not associated with abnormal cavernosal blood gas values, congenital hematologic disorders (i.e., Sickle cell disease), or hematologic malignancy. Non-ischemic priapism is often associated with chronic, well-tolerated erections without full rigidity and often occurs following perineal trauma, intracavernosal injections or aspirations, or any other procedure that can lead to cavernosal artery laceration and subsequent formation of an arteriovenous fistula between the cavernosal artery and lacunar spaces of sinusoidal tissue [110]. Unlike ischemic priapism, non-ischemic priapism is not a medical emergency and roughly 62% of patients will have spontaneous resolution of symptoms without intervention [15]. As such, the initial treatment for patients with non-ischemic priapism is observation for up to six months before considering procedural intervention [15]. Unfortunately, only 60% of the patients whose priapism resolves spontaneously will have full recovery of their erection. In the work-up of all forms of priapism, corporal aspiration and blood gas analysis is performed for diagnostic purposes. However, if non-ischemic priapism is confirmed, therapeutic aspiration and/or sympathomimetic injection is not recommended due to lack of clinical efficacy. If the non-ischemic priapism does not resolve spontaneously within six months or the patient requests treatment, arterial embolization using absorbable (i.e., absorbable gelatin, autologous blood clot) or non-absorbable materials (ethanol, coils, acrylic glue) can be performed [15]. When comparing the use of absorbable vs. non-absorbable embolization materials, studies have demonstrated similar efficacy (74% vs. 78% resolution); however, use of non-absorbable materials was associated with an eight-fold increase in the rate of ED (5% vs. 39%). Hence using absorbable material for embolization, like autologus blood clot, is the best option. Patients who fail embolization therapy may opt for surgical correction, performed with intraoperative color duplex ultrasonography [1]. All patients should be counseled on inherent risks of intervention, as several complications, such as worsening of erectile function, perioperative infection, and failure of embolization to reverse priapism have been reported [21].
Go to :
PENILE PROSTHESIS
Prior to the discovery of oral and injectable intracavernosal therapies like sildenafil and alprostadil, PP was the only recognized treatment option for men with ED [222324]. While PP is now a third-line treatment option for patients with refractory ED, its utility in the early treatment of ischemic priapism has advanced [2526]. Currently, there are two types of PP: malleable (semirigid, non-inflatable) and inflatable penile prostheses (IPP). Malleable prostheses have traditionally consisted of paired silicone or spiral wire core implants, which are inserted into the corpora of the penis. While many variations of malleable prostheses exist today, the most widely used models in the United States are the American Medical Systems (AMS) Spectra implant (Minnetonka, MN, USA) and the Coloplast Genesis implant (Minneapolis, MN, USA); both of which have shown to deliver high levels of patient satisfaction (75.6% and 77.1% for Spectra and Genesis prosthesis, respectively [p=0.497]) [272829]. IPP can be stratified into two- and three-piece models. IPP serve the same function as malleable prostheses with differences only in structural composition. IPP consist of three components: one cylinder located inside each penile corpora, a reservoir placed in different locations depending on the model, and a pump positioned in the scrotum. When a patient repetitively compresses the scrotal pump, the saline-filled reservoir is emptied and the corporal cylinders are filled - mimicking the gradual increase in girth and length observed during a normal erection. The two-piece IPP model has its reservoir located inside the proximal portions of each cylinder. Conversely, the reservoir of the three-piece model, which is larger than the reservoir of two-piece model, is located somewhere in the abdominal space. In comparing the reservoir of two models, a previous study demonstrated that three-piece models were less prone to mechanical failure than their two-piece counterparts (3-piece IPP 6.71%, 2-piece IPP 14.45% [p=0.08]) [30]. However, more recent data suggests similar rates of mechanical failure between the two models. Lux et al [31] and Levine et al [32] reported two-piece IPP mechanical failure rates of 0.7% at 38 months and 2.3% at 22.3 months, respectively, while Kim et al [33] reported a three-piece IPP mechanical failure rate of 2.4% at 36 months. According to Trost et al [34], recommendations regarding the preferential use of any specific model of prostheses are unavailable, but three- piece devices are more commonly utilized when a prosthesis is indicated.
The malleable prosthesis offer benefits such as a simpler surgical procedure, high rates of mechanical reliability, lower cost in comparison to IPP, and ease of use [3536]. However, in addition to the increased complexity of placement of IPP, they have higher patient satisfaction rates than malleable prostheses. This can be attributed to the fact that malleable prostheses are not as cosmetically appealing (difficulties with concealment and partner sensation) as compared to their inflatable counterparts [3738]. IPP offer patients the ability to deflate to a flaccid state and inflate to an erect state when desired. For patients who may have difficulty undergoing immediate IPP placement due to inflammation and fibrosis, use of malleable prostheses as placeholders for future IPP insertion has become a more accepted therapeutic option. Current IPP models carry a 5-year mechanical survival rate ranging from 86% to 96% and a 10-year mechanical survival rate ranging from 67% to 96%, indicating long-term mechanical reliability [3339]. In the past, major complications of IPP included infection and auto inflation; however, design modifications such as antibiotic-coated IPP and lockout valves have lowered these risks to rates below 2% [4041]. In a population-based analysis comparing rates of reoperation between malleable and IPP for infections and non-infectious failures, no significant difference was found between the two groups (7.52% semi-rigid, 7.40% inflatable, p=0.94) [42]. The continued enhancement of IPP and malleable prostheses make both models excellent choices for PP.
1. Penile prosthesis for treatment of refractory ischemic priapism
Ischemic priapism is a condition that requires a timely and individualized treatment in order to obtain the best possible patient outcomes. Following a diagnosis of ischemic priapism, clinicians must evaluate the patient's history, including risk factors, frequency, duration of previous priapic episodes, whether detumescence was achieved spontaneously or after medical or surgical intervention, and baseline erectile function. Studies indicate that the corporal tissue undergoes ischemia and acidosis as early as the sixth hour following the onset of ischemic priapism [43]. If the patient's ischemic priapism presents and resolves within 24 hours of onset, Bennett and Mulhall [44] report that 78% to 100% of these patients regain spontaneous functional erections (with or without phosphodiesterase-5 inhibitor use). Conservative intervention (aspiration/irrigation, pharmacologic intervention) is usually highly efficient in resolving ischemic episodes of this shorter duration [4546]. Of the patients who present at a later time point (>24 hours), Bennett and Mulhall [44] report that only 0% to 44% regain spontaneous functional erections (with or without use of phosphodiesterase-5 inhibitors) even after resolution (Table 2) [44]. Additionally, delayed cases do not usually benefit from conservative intervention and often undergo one of the previously mentioned shunt procedures to treat their refractory ischemic priapism (RIP) [47]. Data suggests that shunt procedures can resolve RIP in 66% to 77% of cases, depending on the shunt used [1]. Patients who fail to achieve detumescence following initial shunting should undergo reoperation to resolve their RIP. Unfortunately, erectile function recovery rates tend to decrease in cases requiring use of higher order interventions (proximal and distal shunts) and ED is often reported even after successful detumescence [4849]. If patients are interested in resuming sexual intercourse following the resolution of their care, they inevitably require PP due to the increased severity of their ED. The early use of PP has become a common treatment option for patients suffering from RIP [25475051]. The benefits of PP for treatment of RIP patients include resolution of penile pain, prevention of additional corporal fibrosis, maintenance of penile length by preventing loss of length secondary to added corporal fibrosis, and detumescence if IPP are used [435152]. In light of recent literature and the lack of consensus in defining acute PP placement, it seems to be appropriate to consider insertion within three weeks from onset as acute or early PP intervention. Early PP intervention is recommended because delaying insertion can result in further corporal fibrosis, which can lead to more technically challenging procedures, increased surgical complications, and worse outcomes [255354]. Notably, extensive corporal fibrosis can cause penile shortening and also force surgeons to use smaller cylinders that do not adequately compensate for the loss of penile length and thus lead to lower patient satisfaction [475055]. One drawback to acute insertion of PP is an increased risk of infection when compared to those receiving virgin implants. Ralph et al [25] reported a 6% infection rate in 50 cases of acute insertions while Wilson and Delk [56] reported a 3% infection rate in 823 cases of virgin PP insertions. However, Ralph et al [25] noted that these elevated infection rates are still lower than the 10% infection rate reported in delayed PP implantation cases. Previous shunt procedures are also associated with increased post-surgical infections and, when coupled with corporal ischemic changes common to RIP patients, can increase the risk of distal or proximal perforation of prosthesis [2557]. It is important to note that the risk of distal perforation is exacerbated with the use of malleable prostheses and cylinder oversizing [5758]. Salem and El Aasser [57] reported that placing non-absorbable sling sutures between each cylinder and the surrounding tunica albuginea was one way to hold cylinders in place and prevent a possible distal perforation of the malleable prostheses. Due to these added complications, it is crucial to counsel RIP patients about the risks and benefits of shunt surgery, especially if they wish to continue having regular intercourse and are reasonable candidates for PP surgery.

Table 2
Relationship between length of priapic episode and loss of spontaneous functional erection
| Duration of ischemic priapism | Less than 12 hours | Between 12 and 24 hours | Between 24 and 36 hours | Greater than 36 hours |
|---|---|---|---|---|
| Percentage of men with spontaneous functional erections (with or without use of sildenafil) [44] | 100% | 78% | 44% | 0% |
![]()
2. Which type of prostheses should be used?
No consensus exists regarding which types of prostheses provide better outcomes for early and delayed cases of RIP (Table 3) [4347505759]. Nevertheless, there are studies that support the preferential use of one type of prosthesis in early implantation RIP cases. Zacharakis et al [50] support the use of malleable prostheses because they can preserve penile length without placing responsibility on patients to cycle the device, as must be done with IPP. Zacharakis et al [50] also pointed out the ease of explantation associated with malleable prostheses, which is an important benefit, given the possibility of infection and other post-surgical complications. For those patients who desire a more natural erection, Zacharakis et al [50] stated that a malleable device can be exchanged for an inflatable device at a later period. This exchange would be acceptable, as patients will have already benefitted from the length preservation associated with malleable prostheses. However, to avoid the need for additional procedures and the risks and costs associated with them, Sedigh et al [47] proposed that IPP can be a viable option as a first-line treatment for RIP. Apart from the cosmetic superiority of IPP, Sedigh et al [47] reasoned that risks such as penile shortening and infections can be combated with appropriate modifications including, but not limited to, cylinder oversizing and the use of antibiotic-coated prostheses.
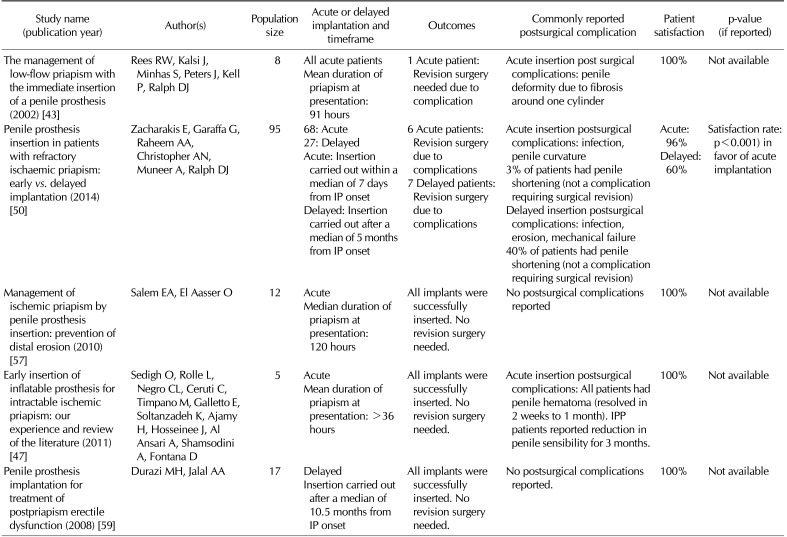
Table 3
Comparing outcomes, complications, and patient satisfaction of studies involving early and delayed penile prosthesis insertion for treatment of ischemic priapism
| Study name (publication year) | Author(s) | Population size | Acute or delayed implantation and timeframe | Outcomes | Commonly reported postsurgical complication | Patient satisfaction | p-value (if reported) |
|---|---|---|---|---|---|---|---|
| The management of low-flow priapism with the immediate insertion of a penile prosthesis (2002) [43] | Rees RW, Kalsi J, Minhas S, Peters J, Kell P, Ralph DJ | 8 | All acute patients | 1 Acute patient: Revision surgery needed due to complication | Acute insertion post surgical complications: penile deformity due to fibrosis around one cylinder | 100% | Not available |
| Mean duration of priapism at presentation: 91 hours | |||||||
| Penile prosthesis insertion in patients with refractory ischaemic priapism: early vs. delayed implantation (2014) [50] | Zacharakis E, Garaffa G, Raheem AA, Christopher AN, Muneer A, Ralph DJ | 95 | 68: Acute | 6 Acute patients: Revision surgery due to complications | Acute insertion postsurgical complications: infection, penile curvature | Acute: 96% | Satisfaction rate: p<0.001) in favor of acute implantation |
| 27: Delayed | 7 Delayed patients: Revision surgery due to complications | 3% of patients had penile shortening (not a complication requiring surgical revision) | Delayed: 60% | ||||
| Acute: Insertion carried out within a median of 7 days from IP onset | Delayed insertion postsurgical complications: infection, erosion, mechanical failure | ||||||
| Delayed: Insertion carried out after a median of 5 months from IP onset | 40% of patients had penile shortening (not a complication requiring surgical revision) | ||||||
| Management of ischemic priapism by penile prosthesis insertion: prevention of distal erosion (2010) [57] | Salem EA, El Aasser O | 12 | Acute | All implants were successfully inserted. No revision surgery needed. | No postsurgical complications reported | 100% | Not available |
| Median duration of priapism at presentation: 120 hours | |||||||
| Early insertion of inflatable prosthesis for intractable ischemic priapism: our experience and review of the literature (2011) [47] | Sedigh O, Rolle L, Negro CL, Ceruti C, Timpano M, Galletto E, Soltanzadeh K, Ajamy H, Hosseinee J, Al Ansari A, Shamsodini A, Fontana D | 5 | Acute | All implants were successfully inserted. No revision surgery needed. | Acute insertion postsurgical complications: All patients had penile hematoma (resolved in 2 weeks to 1 month). IPP patients reported reduction in penile sensibility for 3 months. | 100% | Not available |
| Mean duration of priapism at presentation: >36 hours | |||||||
| Penile prosthesis implantation for treatment of postpriapism erectile dysfunction (2008) [59] | Durazi MH, Jalal AA | 17 | Delayed | All implants were successfully inserted. No revision surgery needed. | No postsurgical complications reported. | 100% | Not available |
| Insertion carried out after a median of 10.5 months from IP onset |
![]()
3. Surgical management of corporal fibrosis
In cases of delayed implantation, the increased surgical difficulty associated with placing any kind of prosthesis inside the fibrotic corpora is a factor that should not be overlooked. In such cases, the insertion of malleable or inflatable cylinders into the fibrotic corpora is equally challenging and, thus, the preferential choice of prostheses in these cases needs to be based on other indications. Experienced surgeons can mitigate the challenges of fibrotic corpora by performing multiple corporotomies, resecting scar tissue either via a transcorporal or open approach, utilizing a cavernotome to avoid openly resecting the scar tissue, and using implants with smaller diameter cylinders, such as AMS CXR and Coloplast narrow base IPP [5360616263]. Martínez-Salamanca et al [53] describe the wide excision of scar tissue (excavation), a technique involving the surgical removal of the fibrotic tissue from the surrounding tunica albuginea by extension of the penoscrotal incision and corporotomy, as the classic approach to managing fibrotic corpora in the placement of PP.
Generally speaking, a stepwise approach is recommended to manage anticipated penile curvature. The surgeon can attempt to place and inflate the cylinders and following an assessment of residual curvature, manual modeling can be performed and stopped if the residual curvature is <30°. Plaque-releasing incision(s) can be considered if residual curve >30°, and, finally, tunical graft needs to be considered if tunical defect >2.0 cm. New developments such as vacuum therapy are also making PP implantation into fibrotic corpora surgically amenable [64].
Currently, the selection of prosthesis for both early and delayed RIP patients is largely based on patient desires, cost, insurance coverage, and the surgeon's experience with each type of PP. The preferential use of one type of prosthesis for early and delayed RIP cases is still a point of contention. More studies comparing outcomes of each type of prosthesis in early and delayed RIP cases would assist with patient and physician clinical decision-making.
4. The psychological impact of early penile prostheses placement in refractory ischemic priapism
While the advantages and disadvantages of early PP intervention have been well documented and continually investigated, the psychological effects on RIP patients who must quickly decide to undergo PP surgery and then accept the results, is an understudied topic. By raising awareness that PP surgery is an optimal treatment for RIP, more at-risk patients will be preemptively aware that they may potentially need PP surgery down the line. Currently, some providers advocate to delay the procedure for up to one week to give patients time to better understand their situation and have reported less-challenging PP insertion even after this delay [47]. Whether or not most providers advocate for allowing patients such a period of time, or if such a period of time is enough for patients to sufficiently comprehend their situation and become comfortable with their ultimate decision, remains unknown [65]. Although it is evident that delayed treatment increases corporal fibrosis, if the possible psychological benefits of an increased window of time outweigh the negative physical effects, such a delay may be justified. Randomized controlled trials would significantly assist our understanding of this topic, but due to the acuteness and rarity of priapism, it is very difficult to design a well-powered randomized controlled trial.
Go to :
CONCLUSIONS
PP is a treatment option for ischemic priapism-induced ED, whether anticipated or established. Current guidance is based on evidence from consensus expert opinion and small-sized retrospective clinical studies. The ongoing debate regarding the type of prosthesis and timing of implantation will most likely continue, in the absence of randomized controlled trial-derived high level evidence. A patient-centered approach and joint decision-making based on the current evidence seems to be a reasonable approach for now for men with RIP.
Go to :
 XML Download
XML Download