

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There are many grey areas in the field of penile rehabilitation after radical prostatectomy (RP). For this reason, the recovery of spontaneous erectile function after RP remains a challenge for physicians [1]. Even if oral phosphodiesterase type 5 inhibitors (PDE5i) are the first-line therapy for erectile function recovery, no gold-standard oral treatment has been approved. Many schedules with various timing and dosage parameters have been proposed and used with different results in terms of efficacy and patients' compliance [2]. Nonetheless, approximately 15% to 80% of all patients undergoing RP do not respond to oral treatment for erectile dysfunction (ED) and require intracavernous therapies [3]. On one hand, the clinical efficacy of intracavernous therapy has been demonstrated in the setting of rehabilitation after RP, and it is one of the most commonly used approaches [2]; on the other hand, a significant number of patients treated with intracavernous therapy show sub-optimal compliance [3], and a third of patients dropped out from the treatment [4]. The failure of spontaneous erectile function recovery is caused by penile fibrosis and penile shortening [5]. In such cases, implanting a prosthesis is the only possible treatment option for recovering the patient's penile erection and restoring the patient's sexual quality of life (QoL). In most cases, a penile prosthesis implant is usually placed at least 2 to 3 years after RP, when the corpus cavernosum fibrosis associated with functional inactivity has already irreversibly damaged the erectile tissue. For this reason, about 20% to 30% of patients consider their penile implants to be “unsatisfactory” [67]. To overcome this issue, Khoudary et al [8] performed the first simultaneous placement of a penile prosthesis during open RP in 1997, aiming at an early return to sexual function. This procedure has been performed without any impact on oncological outcomes and without significant adverse effects. Herein, we describe a case series of patients who underwent laparoscopic extraperitoneal RP combined with simultaneous penile prosthesis implantation (PPI) and evaluate the impact of this treatment strategy on preserving the full dimensions of the penis and improving patients' sexual QoL.
Go to : 
MATERIALS AND METHODS
1. Study population and study schedule
In this retrospective study, we evaluated a series of 10 patients who underwent simultaneous PPI and RP between June 2013 and June 2014. All clinical, anamnestic, and demographic data were collected at the time of surgery. Moreover, data regarding QoL and sexual function were collected using dedicated questionnaires. All procedures were performed according our standard practice. All patients and their partners underwent sexual counselling with a clinical sexologist, both before surgery, in order to assess their motivation to undergo such a procedure, and after surgery, in order to investigate their level of satisfaction with the results.
The present study was based on a case series of patients who had received a similar treatment and whose medical records, treatment exposures, and outcomes were analysed retrospectively, with a descriptive analysis only. The study was conducted in line with the STROBE statement (http://www.strobe-statement.org) [9]. Due to the retrospective nature of the study and the fact that fosfomycin trometamol has been approved for the treatment of urinary tract infections in Italy, the study did not require approval by the local ethics committee. Nevertheless, our study was conducted in line with the Good Clinical Practice guidelines and the ethical principles laid down in the latest version of the Declaration of Helsinki.
2. Data collection
All patients were evaluated at outpatient visits with penile measurements and questionnaires which were administered, before surgery, at discharge from the hospital, on postoperative days 21 to 28, each 3 months for the first year, and each 6 months thereafter. Moreover, at the time of surgery, the following parameters were recorded: the patient's and partner's age, the Charlson comorbidity index, preoperative prostate-specific antigen levels, Gleason score, penile length, clinical prostate cancer stage (through an abdominal computed tomography [CT] scan and skeletal scintigraphy), estimated blood loss, visual analogue scale (VAS) pain scores, analgesic use, duration of hospital stay, and surgical complications. Moreover, surgical complications were recorded according to the Clavien-Dindo classification.
3. Penile length measurements
Penile length was evaluated through a manual measurement of the fully stretched penis in the flaccid state. The length was obtained from the pubis to the tip of the penis. All measurements were made in centimetres.
4. Questionnaires
Patients completed dedicated questionnaires for patient satisfaction and the 36-Item Short Form Health Survey (SF-36) questionnaire [10]. Patient satisfaction was evaluated using patient-reported outcomes (PROs) [11]. Patients' QoL was measured using an Italian version of the SF-36 Health Survey, a test particularly suitable for chronic conditions. Moreover, a year after surgery, patients and their partners were also asked to rate their level of sexual satisfaction on a scale of 1 to 10, with 1 meaning “completely unsatisfactory” and 10 meaning “maximum level of satisfaction.” We decided to use the PROs tool instead of the International Index of Erectile Function questionnaire because the aim of the present study was to evaluate the impact of laparoscopic extraperitoneal RP with simultaneous PPI on patients' satisfaction.
5. Inclusion and exclusion criteria
For the present study, we selected all patients who had an indication for nerve-sparing/non-nerve-sparing RP who underwent simultaneous PPI (combination procedure), pre-existing ED, a contraindication for PDE5i or previously documented non-response to PDE5i, and a stable relationship for at least 6 months. Moreover, we selected only patients who failed or declined to use intracavernous therapies.
6. Surgical procedure
All laparoscopic RP procedures were performed by a single experienced uro-oncological surgeon (RB). All penile prostheses were placed by a single surgeon with high-volume experience in PPI surgery (NM) [8]. Upon conclusion of the prostatectomy, and after removing the prostate via access through a Hasson trocar, we manually positioned the reservoir. The pneumo-Retzius was re-determined and the positioning of the reservoir optimized between the bladder and pubis. We then made a penile-scrotal incision, and isolated the internal inguinal ring with a blunt incision as far as the external fascia of the rectal-abdominal muscles that was crossed by fine-tip forceps, the path of which was simultaneously monitored from the laparoscopic access. The reservoir tube, previously plugged with a special titanium plug, was then dislocated to the penile-scrotal incision. The reservoir was then inflated and its location checked once again. A pelvic drain was positioned and removed on day 1. After ensuring haemostasis, the implant was positioned. Initially, the 2 cylinders were positioned following bilateral cavernosotomy, followed by the pump at the level of the scrotum, and subsequent connection of the tubing. The prosthesis was then almost fully activated for the first 24 hours with a compressive bandage. All patients stayed for 4 hours in a nurse-operated recovery room [12]. The drain was removed on day 1 and patients were discharged from the hospital on day 4. On day 10, retrograde and voiding cystography was carried out after removing the bladder catheter. Activation of the prostheses took place between day 21 and day 28. All steps of the procedure are presented in Figure 1.

7. Ethical considerations
The present study was conducted as a consecutive case series, in which patients who received a similar treatment were followed and all outcomes were recorded and analysed. Even though the case series had a descriptive study design, the local ethical committee was informed about the study.
Go to :
RESULTS
Ten patients, with a median age of 61 years (range, 56–65 years), underwent laparoscopic extraperitoneal RP with simultaneous PPI by a single urologist (NM) in the study period and completed follow-up. Their respective partners had a median age of 50 years (range, 27–61 years). All clinical, laboratory, and demographic characteristics at the time of surgery are displayed in Table 1.
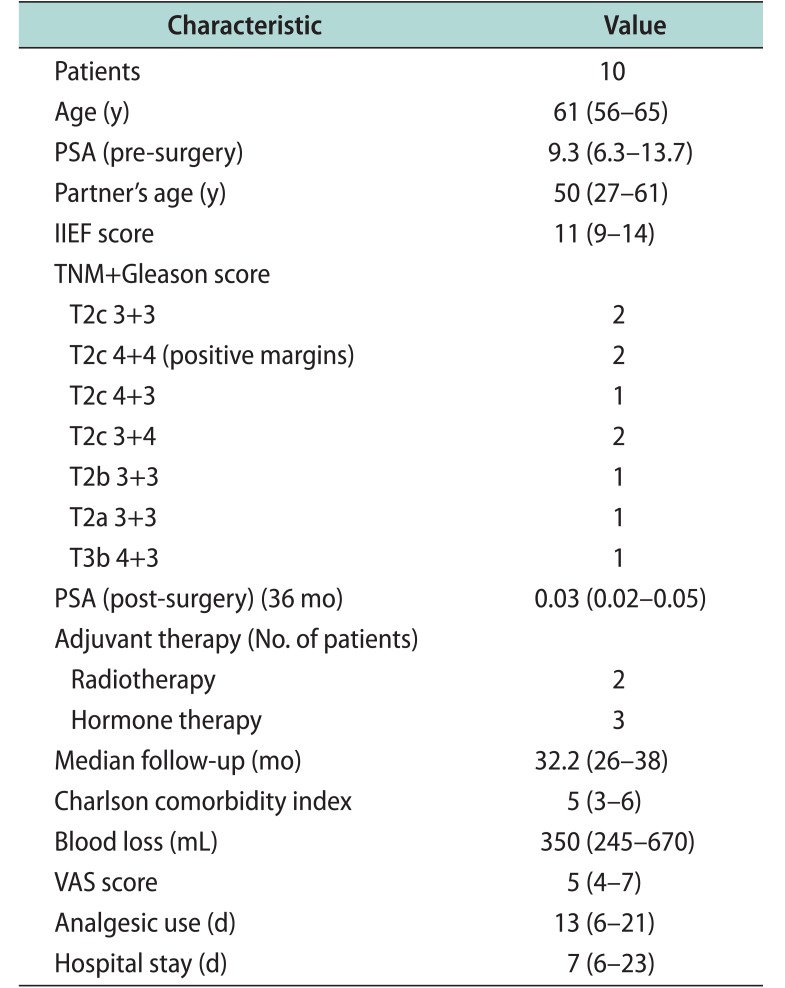
Table 1
Clinical, laboratory, and demographic characteristics
![]()
1. Surgical complications
According to the Clavien-Dindo classification, 1 patient reported a severe complication: migration of the reservoir into the bladder, which was resolved without prosthesis removal. This complication occurred even though the reservoir had been placed under vision. A CT scan was carried out, and it demonstrated a lesion on the superior wall of the bladder due to a pressure ulcer formed by the reservoir near a bladder diverticulum. The reservoir was then removed from the bladder and changed through laparotomic access. The bladder wall was then repaired and a catheter was placed. After 7 days, the catheter was removed and the patient was discharged after cystography. No prosthesis infections occurred. Table 1 presents the duration of analgesic therapy (1,000 mg tablets of paracetamol) and the median VAS scores during hospitalization.
2. Oncological outcomes
Over a median follow-up of 32.2 months (range, 26–38 months), 7 patients were disease-free without adjuvant therapy, and 3 were on hormonal therapy; 2 of the latter group had to undergo radiotherapy after surgery (Table 1).
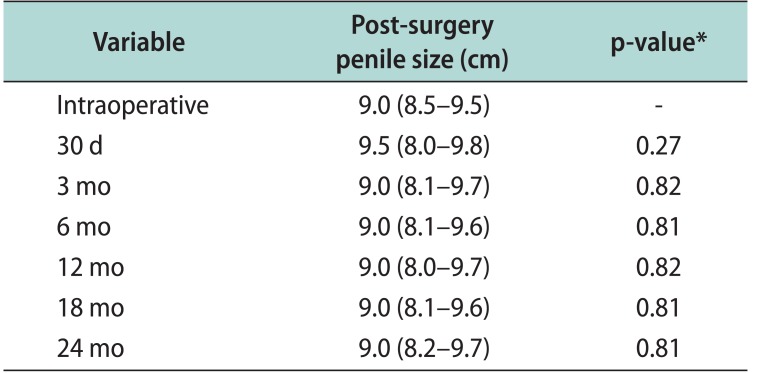
3. Penile length at the time of surgery and at the follow-up visits
The median penile length at the time of the surgery was 9 cm. Post-surgery penile size measurements showed the preservation of the full dimensions of the penis compared to the preoperative measurements (Table 2). No statistically significant differences were found between the preoperative penile length measurements and the follow-up measurements (Table 2). Furthermore, a reduction of 0.5 cm was observed in only 20% of the patients, but no patients described having problems with their penile dimensions.
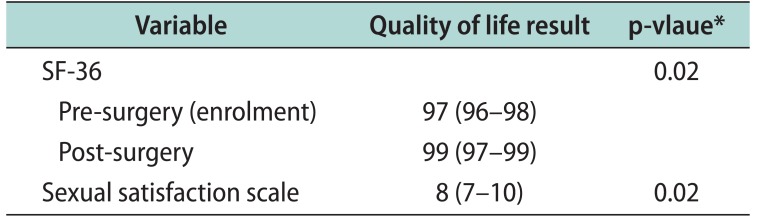
4. Quality of life evaluation
The pre-surgery SF-36 median value was 97 (range, 96–98). According to post-surgical sexual counselling with a clinical sexologist, all patients were satisfied with their penile implants, and the couples' level of sexual satisfaction was rated median of 8 (range, 7–10). The median post-surgery SF-36 score was 99 (range, 97–99) (Table 3). A statistically significant difference was found between the pre-surgery and post-surgery SF-36 scores (p=0.02) (Table 3).
Go to :
DISCUSSION
1. Main findings
Post-surgical ED is a risk factor in RP. In this case series, we aimed to evaluate the effects of simultaneous penile implant placement during RP on penile length, and observed interesting results that should be considered in future studies.
Our case series demonstrated that, in selected and very motivated patients, it is possible to perform laparoscopic extraperitoneal RP with simultaneous PPI, with few complications (10%) and with good level of satisfaction among patients and their partners.
2. Results in the context of previous reports
In the 1990s, Clough et al [13] suggested the integration of plastic surgery techniques with breast-conserving treatments for breast cancer. Conceptually, this approach was referred to as oncoplastic surgery, which aims at providing safe oncological treatment through careful preoperative planning and the incorporation of plastic surgery techniques, in order to obtain good oncological control with favourable cosmetic results in cases of large breast volume and large tumours [14]. In the urological setting, RP offers an attractive opportunity for tumour removal, either as a form of definitive management or as the first step in multimodal therapy [123456789101112131415]. Furthermore, bilateral nerve sparing, usually carried out in low-risk cases of cancer, is often associated with an increased risk of positive surgical margins in patients with pathologic T2 disease during RP [16]. For this reason, patients who report ED even before surgical treatment should undergo non-nerve-sparing surgery. These 2 types of patients are the ideal candidates for simultaneous laparoscopic RP and PPI. The main goal of surgery is usually to achieve an oncological cure, regardless of the preservation of sexual function, which can be restored later by intracavernous therapies or by PPI [1]. In this context, Khoudary et al [8] performed a combination procedure of open non-nerve-sparing radical retropubic prostatectomy and placement of a penile prosthesis in 50 men. This group was compared with a group of 72 men who went RP alone during the same time interval. No significant differences were noted in the preoperative patient variables. The mean operative time for prosthesis insertion was 82 minutes, and the mean time to sexual intercourse was 12.7 weeks. No prosthesis infections occurred, with a mean follow-up of 1.7 years. Four men (8%) required revision of their inflatable penile prosthesis. There were no significant differences between the combination procedure and RP alone with regard to estimated blood loss, length of hospital stay, or analgesic use [8]. Men who chose the simultaneous placement of a penile prosthesis with RP reported greater overall QoL [91718]. In our study, post-surgery penile size measurements showed the preservation of the full dimensions of the penis compared to the preoperative measurements. No prosthesis infections occurred, over a median follow-up of 32 months. In light of these results, laparoscopic extraperitoneal RP with simultaneous PPI could be proposed to selected and very motivated patients because:
a) Medicated AMS InhibiZone (American Medical Systems, Inc. [AMS], Minnetonka, MN, USA) penile prostheses reduce the risk of prosthesis infections. Moreover, the extraperitoneal approach is preferable in order to keep the prosthesis reservoir located in a place with a low risk of infection;
b) Simultaneous PPI preserves penile length; and
c) The combined procedure reduces the duration of hospitalization and allows patients to quickly resume sexual activity. A faster return to a satisfactory sexual life could have a positive impact on QoL and on the couple's well-being.
3. Strengths and limitations of the study
Some aspects of this study should be taken into account, in particular the fact that all surgical oncological procedures were performed by a single dedicated surgeon and all prosthesis implantations were performed by the same surgeon with a high-volume experience. Moreover, the psychological counselling support and the involvement of the partner in the surgical decision-making process should be considered strengths of this study. The main limitation of this study is the fact that it was a consecutive case series. However, our findings could serve as a basis for planning future studies. The majority of our patients had low- or intermediate-risk cancers and they could have undergone complete nerve-sparing resection, which in experienced hands, does not result in high positive margin rates. However, all patients reported stable ED with no benefits from PDE5i or intracavernous therapy. For this reason, we did not consider this treatment strategy to be overtreatment. Finally, the inclusion of a psychologist in the patients' care should be considered a strength of this study. Psychological support during the PPI is a key means of improving adherence to the follow-up and overall outcomes.
4. Implications for clinical practice
We believe that laparoscopic extraperitoneal RP can be considered an optimal surgical technique that offers considerable safety margins for the simultaneous implantation of a tricomponent penile prosthesis, even though simultaneously performing 2 surgical procedures may increase the risk of complications. The hospitalization length is no longer than that required for normal surgery, and the additional costs of the prostheses can be easily amortized by avoiding the costs of a second surgical operation for the penile implant and avoiding the postoperative use of prostaglandins for penile erection.
The main complications of prostate cancer surgery are ED and urinary incontinence. Several patients received an artificial sphincter for urinary incontinence. The presence of a penile implant is not a contraindication for artificial sphincter implantation. The cuff can be placed through the perineal approach in the bulbar urethra or over the bladder neck in particular cases. The reservoir can be placed on the opposite site of the penile implant reservoir and the pump in the opposite part of the scrotum. This possibility should be taken into account in the management of these patients.
Go to :
 XML Download
XML Download