

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Decreased physical function is a representative sign of frailty in elderly people [1], which is usually accompanied by a decrease in testosterone levels in elderly men [2]. Lower testosterone levels are associated with decreased physical function and increased mortality [3], and frailty is associated with decreased quality of life [4]. However, there is no effective clinical treatment to restore physical function in the elderly. One of the mechanisms for the decreased physical function in the elderly is sarcopenia [5], and especially in elderly men, muscle mass is associated with testosterone levels [6].
Although many randomized controlled trials (RCTs) of testosterone replacement therapy (TRT) have been performed, these studies generally had small sample sizes and a variety of study designs, and the effects of TRT on improving physical function are equivocal [789]. While in one study [7] testosterone supplementation improved strength and was suggested to have a role in the treatment of frailty in hypogonadic males, another study [8] did not observe any increase in muscle strength, but only an increase in muscle mass.
Some systematic reviews (SRs) [10111213] investigating the effects of TRT on the body have been published. However, one study [10] included middle-aged subjects and did not include recent studies. Although another study [13] performed a comprehensive SR including elderly men, the heterogeneity in the target groups and outcomes was large, and no significant conclusions were suggested. Accordingly, a quantitative analysis including recently published high-quality RCTs assessing physical function [214] could yield additional clinical significance. Therefore, we conducted a rapid SRs, including elderly men receiving TRT, to assess the effects of TRT on muscle strength and physical function. We also performed quantitative analyses of the outcomes of some RCTs in order to determine their clinical significance. The search strategies and study selection criteria are explained at the end.
TESTOSTERONE REPLACEMENT THERAPY AND MUSCLE STRENGTH
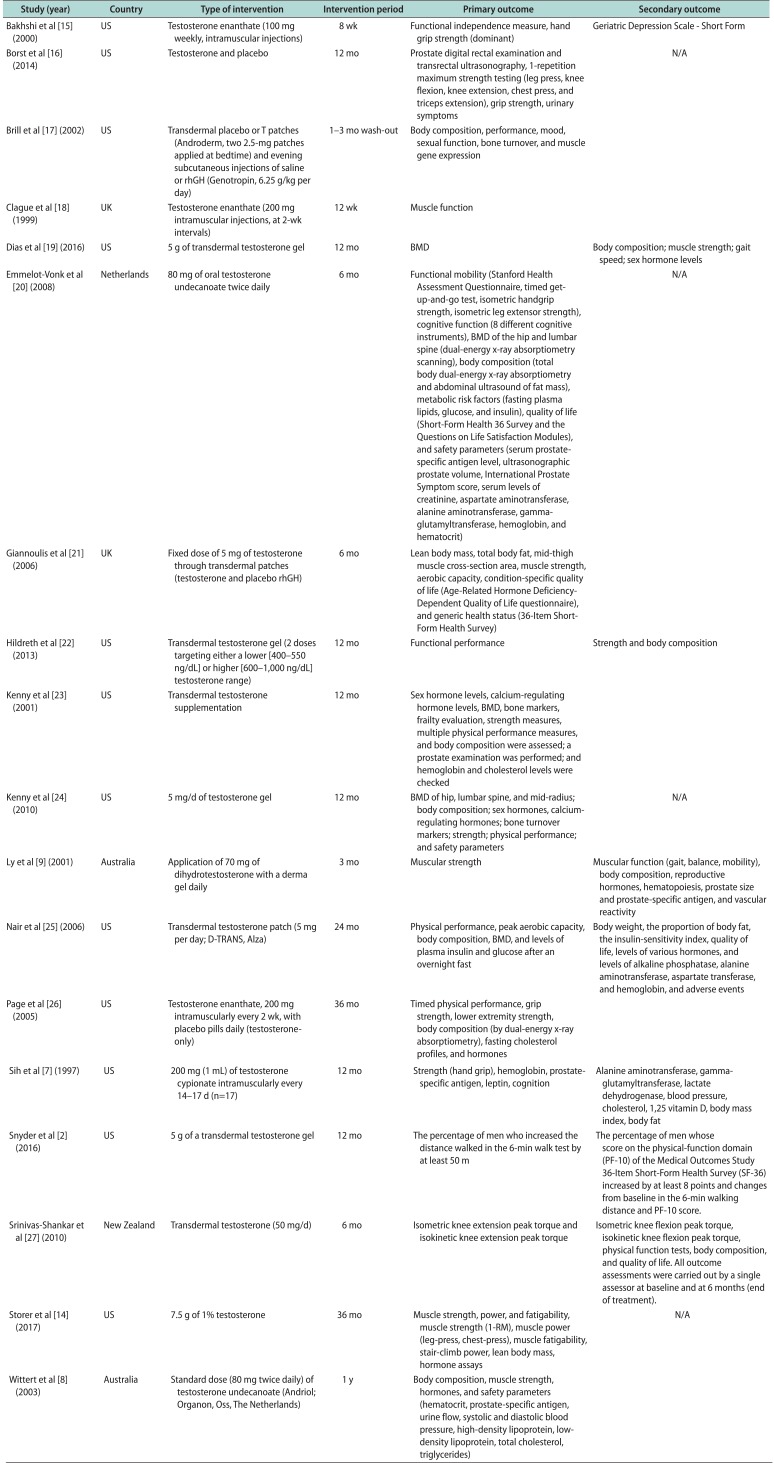
Muscle strength is commonly measured with hand grip strength and the 1-repetition maximum (1-RM) for exercises performed as part of strength testing. Sixteen studies examined the effects of testosterone supplementation on muscle strength. Fourteen studies assessed muscle strength as a primary outcome and 2 as a secondary outcome. The other primary and secondary outcomes investigated in each of the studies are listed in Table 1 [27891415161718192021222324252627]. The most common measurements for muscle strength were hand grip strength and leg muscle strength (knee extension and flexion). Other measurements included single or double leg press, chest press, and triceps extension.
1. Hand grip
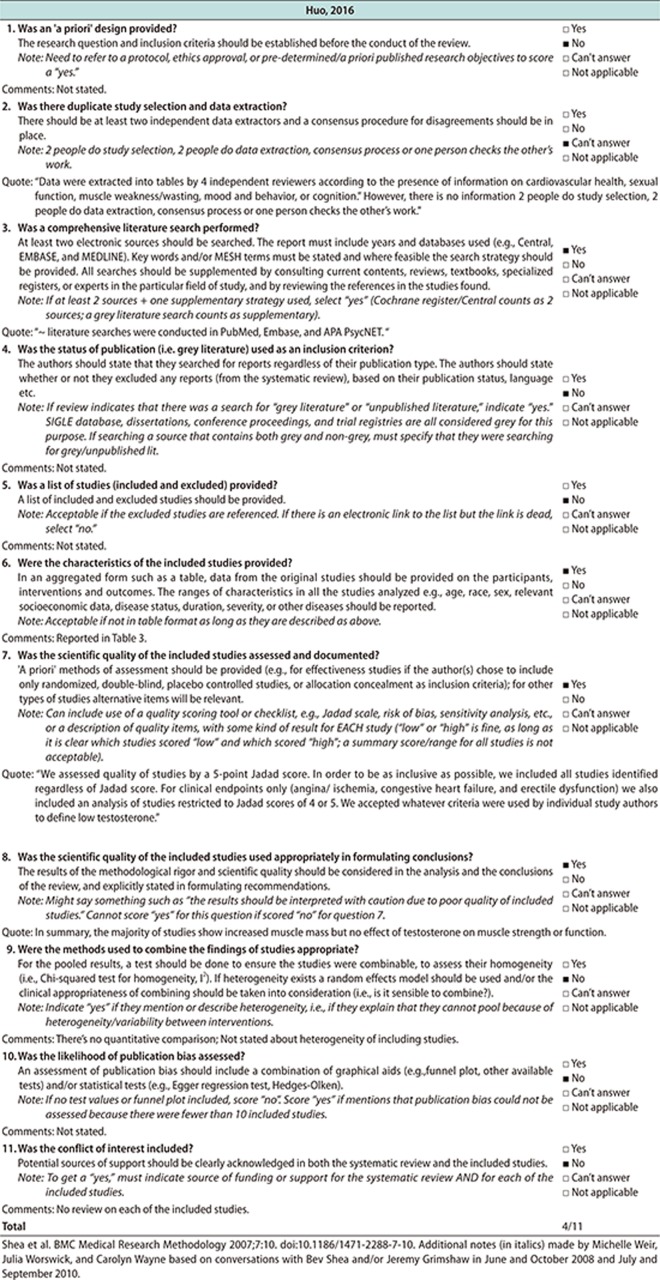
Ten studies included in the analysis measured muscle strength in terms of hand grip strength. Five of these studies were conducted in the United States, 2 in the United Kingdom, 1 in the Netherlands, 1 in Australia, and 1 in New Zealand. A total of 1002 participants were included in the analysis. The intervention period varied from 8 weeks to 1 year. All hand grip strength measurements were expressed in kilograms, except for one study [15], for which a pound-to-kilogram conversion was done for the purposes of our analysis. The overall results (Fig. 1) showed that TRT does not increase hand grip strength. However, individual studies, such as a randomized, placebo-controlled, doubleblind study [15], have found that hand grip strength improved after testosterone administration. Other studies [726] that showed improved hand grip strength after testosterone supplementation could not be included in the analysis because they only presented data in figures.
2. Leg muscle strength
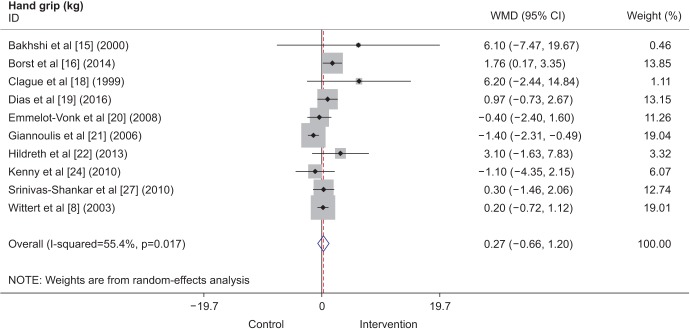
Seven studies included in the analysis measured leg muscle strength. All 7 studies included information for the knee extensor muscles, consisting of a total of 780 participants. Three studies were conducted in the United States, 2 in the United Kingdom, 1 in New Zealand, and 1 in the Netherlands. The study conducted in the Netherlands [20] did not include measurements for the knee flexor muscles, so only 6 of the 7 studies included for the knee extensor analysis were included in the analysis of knee flexor strength. This resulted in a total of 543 participants for the knee flexor analysis. The intervention period varied from 12 weeks to 1 year. Lower muscle strength measurements were expressed as 1-RM in kilograms, newton-meters per second, or watts. Although marginal effects were shown for increased knee extensor strength (Fig. 2), when combined with the outcomes for knee flexor strength, the overall results showed no significant difference.
TESTOSTERONE REPLACEMENT THERAPY AND PHYSICAL FUNCTION
Physical function was commonly measured by the 6-minute walk test [28], the Physical Activity Scale for the Elderly (PASE) questionnaire [29], the physical-function domain (PF-10) of the Medical Outcomes Study 36-Item Short-Form Health Survey [30], a physical performance test (PPT) [31], and the Short Physical Performance Battery (ability to rise from a chair, static balance, and 8-foot walk) [32]. Other tests performed in some studies that were not included in our analyses included the supine-to-stand test [33], and the Get-Up- and-Go test [34].
1. 6-minute walk test
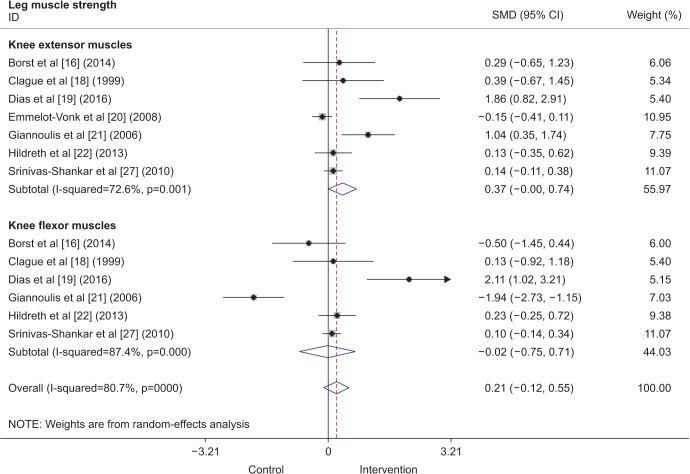
Three studies included in the analysis showed results of the 6-minute walk test. Two of these studies were conducted in the United States, and 1 in New Zealand. A total of 733 participants were included in the analysis. The intervention period varied from 6 months to 1 year. All TRT interventions were done using transdermal testosterone gel, although the dosages differed between studies. The overall results (Fig. 3) showed that TRT improved the 6-minute walking distance by 9.35 m (95% confidence interval [CI], 0.64–18.07 m).
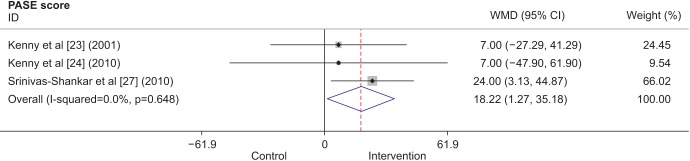
2. Physical Activity Scale for the Elderly score
Three studies included results from the PASE questionnaire [232427], which is known to be a reliable instrument for assessing physical activity in older people [29]. Two studies were conducted in the United States, and 1 was conducted in New Zealand. A total of 504 participants were included in the analysis. The intervention period varied from 6 months to 1 year, and the participants in all 3 studies received transdermal testosterone supplementation. Two studies [2324] administered 5 mg per day for 12 months, while another [27] administered 50 mg per day for 6 months. Even though each of the individual studies did not show statistically significant improvements in the PASE score, when the individual results were combined, the overall results (Fig. 4) showed that there was an increase of 18.22 points (95% CI, 1.27–35.18 points) in the PASE score with TRT.
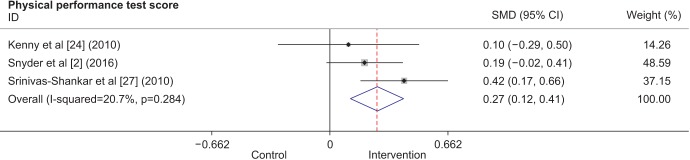
3. Physical performance test
Three studies were combined to analyze the effects of TRT on physical performance. Two studies were conducted in the United States, and 1 was conducted in New Zealand. A total of 733 participants were included. All interventions consisted of transdermal testosterone, and the intervention period varied from 6 months to 1 year. The overall results (Fig. 5) showed improved physical performance after TRT. Other studies that also showed improved physical performance after testosterone supplementation could not be included in the analysis because they only presented data in figures for a timed PPT [26] or gait speed [19] and did not provide exact measurements. Another study did not report outcomes for the functional assessment tests that were conducted, such as maximal reach, standing balance, fast walk, and chair rise [9], and hence, could not be included.
SUMMARY
The overall analyses showed that TRT is not associated with increased muscle strength, whereas it does increase physical function. This is in accordance with previous findings [789]. However, as the number of studies included in some analyses was limited, these results are not generalizable to elderly men in general as a whole. Additionally, most of the reviewed RCTs were conducted in the United States or Europe, and there was no mention of the inclusion of participants from other ethnic backgrounds, such as Asians. Therefore, further studies are needed to investigate the effects of TRT on muscle strength and physical function in populations with a broader ethnic background.
Some difficulties were encountered during the review. For instance, when comparing results for muscle strength, some studies included exercise training and some did not. Moreover, some studies measured isokinetic muscle strength and some measured isometric muscle strength with different dynamometers, which made them difficult to compare. Additionally, the muscle strength evaluation protocols differed for each study. The lack of a standardized, validated exercise protocol to evaluate muscle strength made it difficult to compare the results and suggests that further studies are needed to develop a standardized protocol to be disseminated and widely used.
SEARCH STRATEGIES
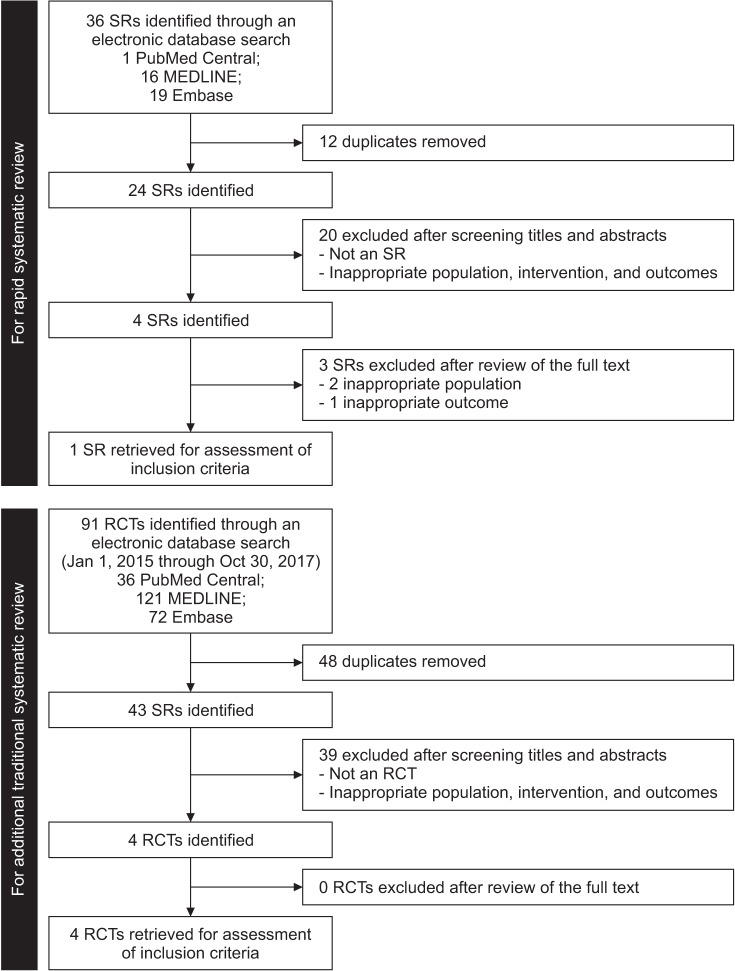
We performed 2 sets of searches, one as a rapid SR and an additional traditional SR, because the latest published SR included studies published up to April 9, 2016. The results for the rapid and traditional SRs and meta-analyses were reported following the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [35] (Fig. 6).
For the rapid SR, the PubMed Central, MEDLINE, and Embase databases were searched for studies published up to October 30, 2017. The initial search was conducted using the following keywords: elderly men aged at least 60 years (for participants), testosterone replacement (for intervention), placebo (for comparison), physical performance (for outcome), and SR (for study design) (see Supplementary Table 1 for the complete list of the search terms). We only included articles published in English. Studies were considered eligible for the rapid SR if they met the following inclusion criteria: 1) being a SR; 2) including elderly men at least 60 years of age; 3) reporting physical function, physical performance, and/or muscle strength; 4) having TRT as the major intervention; and 5) including a comparison with a placebo. Although we searched for healthy elderly men, we did not exclude studies if they included participants with hypogonadism, but studies of other specific diseases, such as diabetes mellitus and Parkinson disease, were excluded from the analysis. We included interventions that compared testosterone supplementation vs. placebo or other substances, such as growth hormone. As a result, 1 SR [13] was retrieved for assessment. The other 3 SRs were excluded because 2 [1011] included inappropriate populations and one [12] had inappropriate outcomes. We then applied AMSTAR [36], a measurement tool for assessing the methodological quality of the retrieved SR, which gave a score of 4 out of 11 (see Appendix 1 for details).
For the additional traditional SR, as the retrieved SR used for the rapid SR included studies between January 1, 1950, and April 9, 2016, we searched for additional RCTs from January 1, 2015, to October 30, 2017 through the PubMed Central, MEDLINE, and Embase databases. We used the same search terms as were used for the rapid SR except for the study design, which was RCTs (see Supplementary Table 2 for a complete list of the search terms). After excluding studies that did not match our inclusion criteria, we included a total of 17 studies and added the 4 RCTs retrieved from the additional search. Subsequently, a total of 21 full-text articles were reviewed for the analysis and 3 studies were further excluded because their population [3738] and outcome measures [39] did not meet our criteria. A total of 18 studies were included in the final analysis.
STATISTICAL ANALYSIS
Statistical analyses were performed using STATA ver. 15.0 (StataCorp, College Station, TX, USA) using the metan command with a random effect. When outcome measurements were given in the same units or the units could be converted, weighted mean differences were calculated, whereas if outcome measurements were given in different, non-convertible units, standardized mean differences were calculated instead.
 XML Download
XML Download