

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Infertility is a common and complex reproductive health problem that is estimated to affect 10% to 15% of couples in industrialized countries, with about half of infertility problems attributable to male factors [1]. Male infertility is associated with a variety of factors itself, including environmental and genetic factors. While the molecular mechanisms underlying the etiology and pathophysiology of male infertility are still largely unknown, the relationship between the reproductive system and the immune system has been found to play an important role in the pathophysiology of male infertility. Fraczek and Kurpisz [2] reported that inflammatory pathologies are among the well-known reasons for male infertility, accounting for 15% of cases. These systemic inflammatory diseases and inflammatory processes may alter sperm function through the production of elevated reactive oxygen species [3]. While the monitoring of cytokines in seminal plasma may improve our understanding of the process that leads to infertility [2], the technical difficulties and costs associated with the use of these inflammatory markers, such as interleukins, tumor necrosis factor-alpha (TNF-α), interferon gamma, and C-reactive protein, in routine clinical practice may limit their use. Alternatively, the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) can be rapidly and inexpensively obtained from a differential white blood cell (WBC) count. The NLR and PLR have already been reported to play a role in inflammatory diseases [45678], but their relationships with male infertility remain unclear. Thus, the aim of our study was to evaluate the association between seminal parameters and inflammation, as measured by the NLR and PLR, among men with abnormal semen analysis and men with normozoospermia.
Go to : 
MATERIALS AND METHODS
Cross-sectional data was collected on male patients from October 2015 to May 2016. The study was approved by the Institutional Review Board of Bağcılar Training and Research Hospital (No. 2015/420) and written informed consent was obtained from all participants. Participants were included if they were older than 18 years old and had either infertility or normozoospermia and a partner with female factor infertility. Patients with normozoospermia who had normal seminal parameters were not considered to be infertile in this study. Baseline characteristics were collected from each patient's medical records and included data on age, body mass index (BMI), smoking, use of anabolic steroids, previous diseases, history of cryptorchidism, medication, and comorbidities. Of the initial sample of 146 men, 18 men were excluded because they presented with varicocele and 12 men were excluded due to hypogonadism, retractile testes, karyotype anomalies, obstruction of spermatic ducts, history of chemotherapy and/or radiotherapy, male accessory gland infection, hematologic disorders, or current steroid therapy. The final sample consisted of 116 participants who were classified into a normozoospermic group (n=59) or an abnormal semen analysis group (n=57) based on the World Health Organization (WHO) guidelines [9].
Semen samples were obtained by masturbation after sexual abstinence for 48 to 72 hours and processed in accordance with the WHO guidelines [9]. The leukocyte concentration was determined using the peroxidase staining technique and sperm vitality was assessed in duplicate using the eosin-nigrosin staining technique [910]. All semen samples that had one or more altered seminal parameters were defined as abnormal, according to the WHO [9]. The complete blood count was obtained by a hematology analyzer (Coulter Gen-S Hematology Analyzer; Beckman Coulter Corp, Hialeah, FL, USA). The total WBC was recorded, along with the neutrophil, platelet, and lymphocyte counts. The NLR and PLR were calculated by dividing the neutrophil count by the lymphocyte count and platelet count by the lymphocyte count, respectively.
The Number Cruncher Statistical System (NCSS) 2007 software (NCSS, Kaysville, UT, USA) was used for statistical analyses. Seminal parameters and baseline characteristics were expressed as mean±standard error of the mean. To compare continuous variables between the 2 groups, the independent t-test was used. For non-parametrically distributed variables, the Mann-Whitney U-test was performed. The Kolmogorov-Smirnov test was used to check the distribution of parameters and the Pearson correlation test was used to assess the degree of correlation among continuous variables. A p-value of <0.05 was considered to indicate statistical significance.
Go to :
RESULTS
Data on the seminal parameters of study participants are shown in Table 1. There were no significant differences in abstinence time, semen volume, liquefaction time, semen pH, or leukospermia between the groups. Sperm concentration, total sperm count, progressive motility, total motility, and normal sperm morphology were significantly greater in the normozoospermic group than in the abnormal semen analysis group (p<0.05).
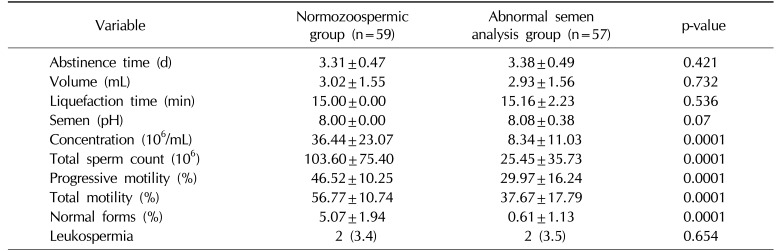
Table 1
Conventional semen parameters of the participants enrolled in this study
![]()
The mean age was 31.04±6.63 years in the normozoospermic group and 30.76±5.81 years in the abnormal semen analysis group. There were no significant differences between the groups with respect to age, BMI, or current smoking status (p>0.05). The NLR was 1.84±0.78 in the normozoospermic group and 1.80±0.75 in the abnormal semen analysis group. The PLR was 95.32±35.47 in the normozoospermic group and 93.57±28.09 in the abnormal semen analysis group. There were no significant differences between the groups with respect to NLR or PLR (p=0.828 and p=0.768, respectively). Likewise, no significant differences were found in the hematologic parameters, including WBC count, neutrophil count, lymphocyte count, and platelet count (p>0.05) (Table 2).
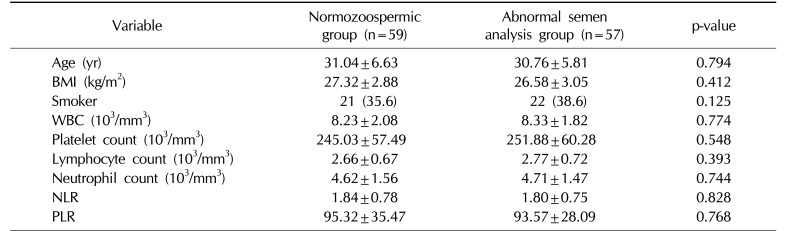
Table 2
Baseline characteristics and hematologic parameters
![]()
The correlation analysis indicated that no seminal parameters were correlated with any hematologic parameters, and no correlations were found among these seminal parameters and the NLR or PLR (Table 3).
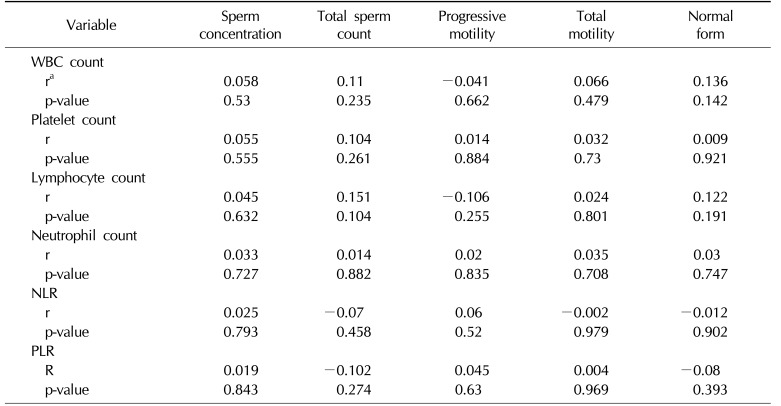
Table 3
Correlation between semen parameters and hematologic parameters
![]()
Go to :
DISCUSSION
The current study is the first to investigate the relationships between seminal parameters and the NLR and PLR, which are inflammatory markers. The findings from our study show that these inflammatory markers are not suitable for screening to identify patients with abnormal seminal parameters.
Previous studies have shown that systemic inflammatory processes are associated with significant alterations in seminal plasma. Disruption of the blood-testis barrier by the inflammatory cytokines TNF-α and interleukin-6 have been found to significantly reduce sperm motility [1112]. Another study revealed that TNF-α was significantly associated with decreased sperm count, sperm motility, and normal sperm morphology among infertile patients [13]. While these inflammatory markers may improve our understanding of infertility, the technical difficulties and costs associated with measuring them in routine clinical practice limit their use. Thus, the aim of the present study was to investigate the relationships between seminal parameters and the NLR or the PLR, which can be determined rapidly and inexpensively.
Neutrophils have several potent effector mechanisms to combat and eventually kill spermatozoa. Oxidative mechanisms that result in the production of reactive oxygen species, the release of several peptides or proteins, and the formation of neutrophil extracellular traps have detrimental effects on seminal plasma [14]. Since neutrophilia and lymphocytopenia occur after systemic inflammation [4], the increase in NLR and PLR found in those with chronic inflammation may also affect seminal parameters.
Additionally, an increase in serum cytokines may have detrimental effects on the hypothalamic-pituitary-testis axis and may negatively modulate testicular function and fertility [15]. In the current study, hypogonadal participants were excluded from the study sample due to the effect of hypogonadism on seminal parameters. The impact of systemic inflammation on these pathways requires further investigations.
The NLR and PLR have been used to detect inflammation in infectious diseases, cardiovascular diseases, various types of malignancies, and several other inflammatory diseases [6781617181920212223]. However, these inflammatory markers have not previously been used to determine the association between inflammation and seminal parameters. In this study, we did not find significant differences in the associations of any of the seminal parameters and the NLR or PLR between the normozoospermic group and the abnormal semen analysis group. Moreover, no significant between-group differences were found in the neutrophil count or the lymphocyte count.
It is difficult to evaluate the reproductive potential of men based on routine seminal parameters alone. Lewis found that only 16% of infertile men and 5% of fertile men showed poor seminal parameters [24]. Systemic inflammation may, therefore, be one cause of male infertility through unknown mechanisms. This study demonstrated that routine seminal parameters were not affected by the inflammatory markers that we studied. There were, however, limitations to our study that are worth mentioning. These include not having the specific fertility status of any of the study participants, as well as having a relatively small sample size. Further research on the associations of seminal parameters with the NLR and the PLR is required to verify the results of our study.
Go to :
CONCLUSIONS
The NLR and PLR can be easily determined in routine practice. However, our study demonstrated that the NLR and PLR were not associated with seminal parameters, and we do not recommend using the NLR or the PLR as markers to screen for abnormal seminal parameters. Consequently, additional large, prospective studies are needed to support our findings and improve the data we have on the relationships of seminal parameters with the NLR and PLR.
Go to :
 XML Download
XML Download