

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The organic causes of erectile dysfunction (ED) include arterial, cavernosal, hormonal, and neurological causes [1]. Arterial ED is associated with atherosclerosis, hyperlipidemia, and hypertension, while cavernosal ED is caused by degenerative changes in the tunica albuginea, degeneration of fibroelastic tissues, and insufficient trabecular smooth muscle relaxation [234]. Hormonal ED may occur in patients with insufficient testosterone or hyperprolactinemia; additionally, alcohol can affect the hypothalamicpituitary-gonadal hormone axis, decreasing testosterone secretion and potentially causing hormone-induced ED [56]. Neurological ED occurs due to central nervous system diseases in the brain and spine, as well as insufficient secretion of neurotransmitters such as acetylcholine and nitric oxide (NO) in components of the peripheral nerve system such as the pudendal or cavernosal nerve [7].
It is known that moderate alcohol consumption increases blood circulation and affects erectile function [8], while chronic alcohol consumption negatively affects erectile function. However, alcohol-induced sexual dysfunction has so far been primarily analyzed as being due to abnormal testosterone levels [9], and the mechanism of how alcohol may directly affect the corpus cavernosum (CC) has not yet been elucidated. This study investigated how alcohol affected CC smooth muscle through an organ bath study of alcohol-administered rabbits and how alcohol affected the CC of rats that received acute and chronic administrations of alcohol.
Go to : 
MATERIALS AND METHODS
1. Study of the effect of acute alcohol administration on the corpus cavernosum
1) Corpus cavernosum organ bath study
Eight while male rabbits (New Zealand, 2.5~3.0 kg) were used. The penis was resected and sections of the CC (2×2×10 mm) were prepared. The thoracic aorta was resected by removing the connective tissue, and the ring (3 mm) was prepared. The CC sections were pretreated with 3 mL of 0.3% 3-[(3-cholamidopropyl)dimethylammonio]-1-propane sulfonate (CHAPS) to detach vascular endothelial cells, manually rubbed for 20 seconds, and then rinsed with Krebs-Henseleit (KH) solution. Vascular endothelial cells were removed by smoothly rubbing the inside of the vessel of the aortic ring with a 25-gauge needle tip. The removal of vascular endothelial cells was confirmed by checking that CC section contraction induced by phenylephrine (PE; 5×10−6 mol) was not prevented by acetylcholine (10−5 mol).
The CC sections and the aortic rings were transferred to the organ bath. One end was connected to the muscle fixation ring and the other end was connected to the isometric tension transducer, and signals were observed and measured via physiography. Chart 5 software (ADInstruments, Bella Vista, Australia) was used to monitor the tension in real time. The KH solution in the organ bath was maintained at 37℃ and a pH of 7.4 by continuously supplying air consisting of 95% O2 and 5% CO2. The initial tension in each section was maintained at approximately 2 g, and the KH solution was replaced every 30 minutes for 2 hours to reach the resting state. The degree of contraction was observed by adding PE after reaching the resting state. Each section was gradually reacted with the PE and increased to the optimal point of the length-tension curve, as determined by the active tension change. The resting state was restored by rinsing with the KH solution 3 times. The tissues were contracted for pretreatment with PE in the organ bath while maintaining the resting optimal isometric tension.
The relaxation response was investigated to assess the CC relaxation mechanism induced by alcohol (0.01%~2%) and acetaldehyde (0.001%~0.1%). The CC was left in the KH solution with the pretreatment drug. The tissues were then contracted with PE to reach the plateau. The following drugs were used for pretreatment: N(G)-nitro-L-arginine methyl ester (L-NAME) (10−5 mol), propranolol (10−5 mol), indomethacin (3×10−5 mol), glibenclamide (10−5 mol), 4-aminopyridine (10−5 mol), and methylene blue (10−5 mol).
2) Electrical stimulation-induced erection study
Forty male white rats (Sprague-Dawley, 280~320 g) were classified into 5 groups depending on the amount of hours that had passed after alcohol administration (n=8 in each group). The rats were placed in the supine position, and blood pressure (BP) was monitored with a polyethylene-50 tube in the carotid artery. The prostate was exposed via a midline incision. In addition, the pelvic nerve plexus was checked. The penis was dissected to the penile crura. The ischiocavernosal muscle around the penile crura was dissected to assess the tunica albuginea in the penis, and a 25-gauge polyethylene-50 tube was inserted in the CC.
The mean arterial pressure (MAP) and intracavernosal pressure (ICP) were measured by the BP manometer transducer and recorder. An electric stimulus was provided with 5 volts for 60 seconds. The pressure before, during, and after the stimulus were measured to assess the hemodynamic response to nerve stimulation. The maximum ICP/MAP percentage was measured by stimulating the cavernosal nerve to assess the response induced by the nerve stimulation and compared across groups.
3) Measurements of cyclic adenosine monophosphate and cyclic guanosine monophosphate in the corpus cavernosum
The penile tissues in the control group and the 2-hour alcohol group were quickly frozen in liquid nitrogen and homogenized in ice-cold 6% trichloroacetic acid. The homogenized tissues were centrifuged for 15 minutes and the cellular proteins in the supernatant were separated in the usual manner. The samples were classified into the control group and the 2-hour alcohol group, and the concentrations of secreted cyclic adenosine monophosphate (cAMP) (n=8) and cyclic guanosine monophosphate (cGMP) (n=8) were measured with an immunoassay. The immunoassay was based on the antagonistic binding method, in which horseradish peroxidase-labeled cAMP and cGMP and fixed amounts of the sample cAMP and cGMP competed for the polyclonal antibody position of the rabbit. The polyclonal antibody was combined to a microplate treated with goat anti-rabbit antibody during the response. It was rinsed to remove excessively binding and non-binding components of the sample, and the substrate solution was added to determine the binding enzyme activity. Absorbance was measured at 450 nm.
2. Study of the effect of chronic alcohol administration on the corpus cavernosum
1) Electrical stimulation-induced erection study
Twelve male white rats were classified into a control group and a 12-week alcohol group (n=6 in each). As an animal model of chronic alcohol administration, 15% alcohol (3 g/kg) was orally administered every day for 12 weeks in the 12-week alcohol group. The same amount of saline was administered with the same method for 12 weeks in the control group. Twenty-four hours after the last administration at 12 weeks, the ICP/MAP percentage was measured using the same method discussed above for the acute alcohol study.
2) Measurement of cyclic adenosine monophosphate and the cyclic guanosine monophosphate in the corpus cavernosum
Changes in the concentration of cAMP and the cGMP in the CC in the control group and the 12-week alcohol group were observed. Twenty-four hours after the last alcohol administration at week 12, levels of cAMP and cGMP were measured using the same method discussed above for the acute alcohol study.
3) Collagen measurement
The mid-part of the penile section in each group was excised and fixed with 10% formalin phosphate-buffered solution. It was then embedded in paraffin, and the samples were excised with a thickness of 4 µm and dyed with Masson trichrome (n=6 in each group).
Collagen was measured using the Sircol collagen assay kit. The frozen penile tissue was excised at thicknesses of 2~3 mm, left in small tubes, mixed well with 1 mg of pepsin including 0.5 mol acetic acid for each 10 mg of tissue and left overnight at 4℃. The next day, the tissues were centrifuged for 60 minutes at 15,000 rpm, the supernatant was filtered with an 0.8-µm pore-size filter, and 200 µL was mixed with 1 mL of Sircol dye reagent and shaken well at room temperature for 30 minutes. It was then centrifuged again, the supernatant was removed, and the remaining material was mixed with 1.0 mL of 0.5 N NaOH, mixed for 5 minutes, and the collagen concentration was measured with a microwell plate reader in the 550-nm range.
4) Immunohistochemical analysis
Sections of CC stored at −70℃ were sequentially precipitated with 10%, 20%, and 30% of sucrose solutions to fix the tissues, and the tissue sections 10 µm in thickness were prepared with an electric frozen slicer. The specific antibody against endothelial nitric oxide synthase (eNOS) was used with a dilution ratio of 1:200 as the primary antibody. The antibody was detected using the avidin-biotin peroxidase technique with diamino benzidine as the chromogen, and the counterstain was performed with H&E.
5) Measurement of endothelial nitric oxide synthase expression with western blotting
The tissues in the 2 CC groups were homogenized using 0.1 mol phosphate-buffered saline (potassium phosphate sodium, pH 7.4) at 4℃ and dissolved in a lysis buffer (5 mmol/L of glycerophosphate, 2 mmol/L of MgCl2, 1 mmol/L of ethylene glycol-bis(β-aminoethyl ether)-N,N, N′,N′-tetraacetic acid (EGTA), 0.5% Triton X-100, 0.5% NP-40, 1 mmol/L of dithiothreitol, and 100 mL of a protease inhibitor cocktail). The protein concentration was measured using a protein assay kit (Bio-Rad, Hercules, CA, USA). Each lane of a sodium dodecyl sulfate polyacrylamide gel was loaded with 25 µg of protein to perform electrophoresis. The separated protein was transferred to a nitrocellulose membrane with a semi-dry transfer unit, and was treated with a blocking solution (5% skim milk/tris-buffered saline-tween [TBST]) at 4℃ overnight to block the intrinsic factors. The eNOS antibody was used as the primary antibody, was allowed to sit for 2 hours, and then the samples were rinsed 3 times for 15 minutes with TBST and treated with the secondary antibody (horseradish peroxidase conjugated goat anti-rabbit immunoglobulin G) for 1 hour. The samples were then developed by being exposed to hyperfilm after a color reaction with a chemiluminescent reagent. The protein standard molecular marker conformed to precision protein standards, the density of each protein was measured using an image analysis program, β-actin density was measured for calibration, and the extent of expression of each protein was surveyed.
6) Data analysis
Statistical significance in the acute alcohol group was assessed using analysis of variance, and comparisons were made with the chronic alcohol group using the Student's t-test. All statistical analyses were performed in PASW Statistics ver. 18.0 (IBM Co., Armonk, NY, USA). p<0.05 were considered to indicate statistical significance.
Go to :
RESULTS
1. Effects of acute alcohol administration on the corpus cavernosum
Alcohol showed a dose-dependent CC relaxation pattern with increasing concentration in the CC. However, it showed a contraction pattern at high concentrations in the aorta. The CC relaxation response was inhibited after pretreatment with propranolol, indomethacin, glibenclamide, and 4-aminopyridine (p<0.05) (Fig. 1).
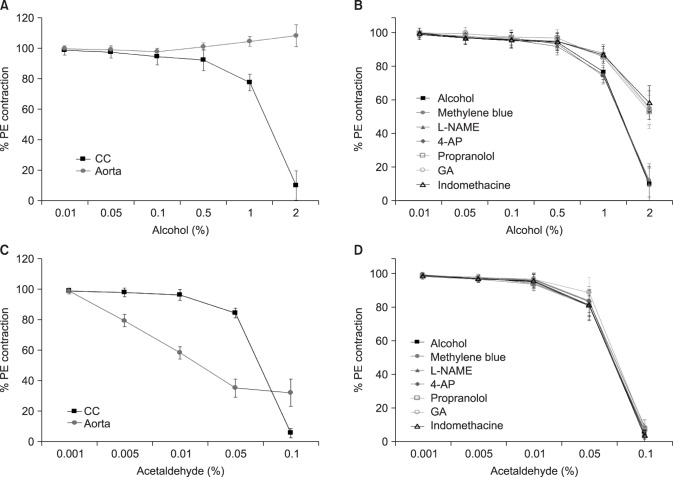 | Fig. 1(A) Effects of alcohol on corpus cavernosum (CC) smooth muscle and the aortic ring in rabbits. (B) Effects of alcohol on the CC smooth muscle after pretreatment with various drugs. (C) Effects of acetaldehyde on CC smooth muscle and the aortic ring in rabbits. (D) Effects of acetaldehyde on the CC smooth muscle after pretreatment with various drugs. PE: phenylephrine, L-NAME: N(G)-nitro-L-arginine methyl ester, 4AP: 4-aminopyridine, GA: glibenclamide.
|
The blood alcohol concentration peaked in the 2-hour alcohol group and the concentration gradually decreased after 2 hours. The ICP/MAP percentage change associated with electric stimulus of the cavernosal nerve after alcohol administration showed a similar pattern, as the blood alcohol concentration and the greatest ICP/MAP percentage increase were observed in the 2-hour alcohol group, in which the blood alcohol concentration was highest (p<0.05) (Fig. 2).
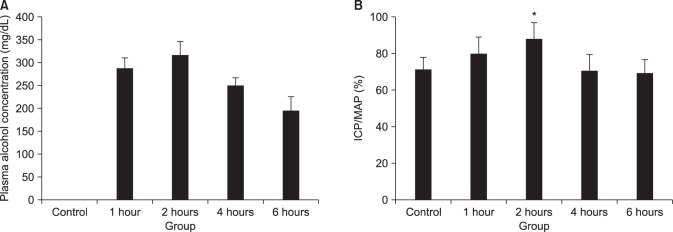 | Fig. 2(A) Changes of plasma alcohol concentration after alcohol administration. (B) ICP/MAP percentage changes during cavernosal nerve electrical stimulation after alcohol administration. *Significant difference from the control group (p<0.05). ICP/MAP: intracavernosal pressure/mean arterial pressure.
|
The cAMP concentration in the CC of the control group was 4.57±1.1 pmol/mL, whereas it was 13.30±4.9 pmol/mL in the 2-hour alcohol group (p<0.05). The cGMP concentration in the CC of the control group was 0.36±0.5 pmol/mL, while it was 0.59±0.5 pmol/mL in the 2-hour alcohol group; however, this difference was not significant.
2. Effects of chronic alcohol administration on the corpus cavernosum
The ICP/MAP percentage associated with cavernosal nerve stimulation in the control group was 84.0%±4.0%, while it was 88.5%±6.5% in the 12-week alcohol group; however, this difference was not significant.
The cAMP concentration in the CC of the control group was 3.04±1.7 pmol/mL, whereas it was 3.42±1.3 pmol/mL in the 12-week alcohol group. This difference was not statistically significant. The cGMP concentration in the CC of the control group was 0.54±0.4 pmol/mL, and 0.33±0.2 pmol/mL; however, this difference was not significant.
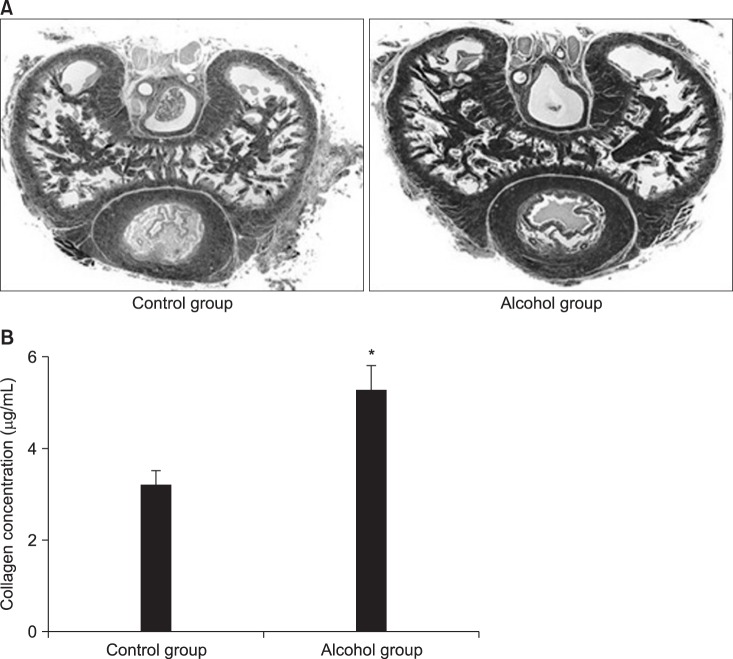
Masson trichrome staining indicated that the 12-week alcohol group showed significantly less smooth muscle in the CC than the control group. The collagen level was significantly higher in the 12-week alcohol group than in the control group (4.77±1.05 µg/mL vs. 3.17±0.23 µg/mL; p<0.05) (Fig. 3).
In the immunohistochemical analysis, eNOS expression was observed in the endothelial cells in the subepithelial capillary in the control group. The response region was the same but the level decreased in the 12-week alcohol group. Western blotting found that the 12-week alcohol group exhibited significantly less eNOS expression than the control group (p<0.05) (Fig. 4).
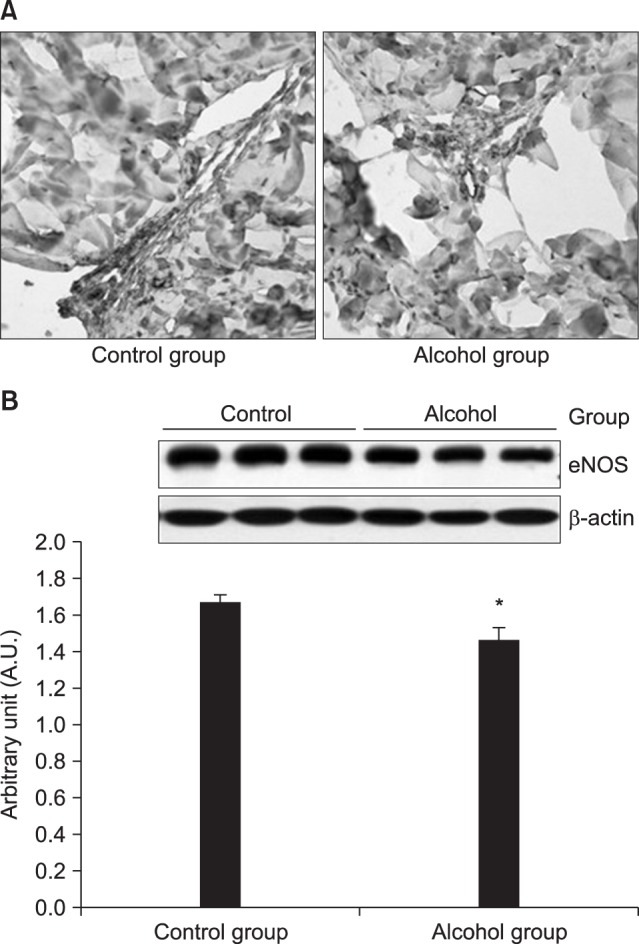 | Fig. 4(A) Immunohistochemical stain of endothelial nitric oxide synthase (eNOS) in the control group and 12-week alcohol group. Representative ×400 sections from the corpus cavernosum (CC) of each rat are shown. The expression of eNOS in CC smooth muscle is indicated using the color brown. Immunoreactivity for eNOS was detected in the endothelial cells of blood vessels. (B) Western blot analysis of eNOS in the control group and the 12-week alcohol group. In the 12-week alcohol group, the expression of eNOS was significantly lower than in the control group. The lower panels denote the means±standard deviations for 3 experiments for each condition determined by densitometry relative to β-actin. *Significant difference from the control group (p<0.05).
|
Go to :
DISCUSSION
Alcohol caused dose-dependent CC relaxation in the CC smooth muscle of rats. However, it led to contraction at high concentrations in the aorta. This confirms that alcohol led to the smooth muscle contraction in the systemic response to a certain extent, but was associated with relaxation in the CC.
Contraction in the CC takes place if adrenergic α-receptors are activated, while relaxation occurs if adrenergic β-receptors are activated [101112]. In our study, the effect of alcohol on CC relaxation was significantly inhibited by pretreatment with propranolol, which is an adrenergic β-receptor blocker, and we therefore suggest that acute alcohol administration caused CC relaxation through the activation of β-receptors.
Arachidonic acid is degraded to prostaglandins by cyclooxygenase in CC smooth muscle, affecting the mechanism of erection through various pathways. Prostaglandin inhibits norepinephrine secretion from the adrenergic nerves in the penis and increases the intracellular cAMP concentration in CC smooth muscle [1314]. This process reduces the intracellular Ca2+ concentration and leads to erection by enhancing smooth muscle relaxation. Our study showed that the effect of alcohol on CC relaxation was significantly inhibited by pretreatment with indomethacin, which is a cyclooxygenase inhibitor, and we therefore suggest that acute alcohol administration led to CC relaxation through the activation of cyclooxygenase.
K+ channels play a role in adjusting the tone of CC smooth muscle [1516]. Hyperpolarization occurs if the K+ channels are activated and opened, which inhibits Ca2+ channel activation, reduces the intracellular Ca2+ concentration, and causes CC smooth muscle relaxation [1718]. Our study found that the effect of alcohol on CC relaxation was significantly inhibited by pretreatment with glibenclamide, which is a KATP channel inhibitor, and 4-aminopyridine, which is a membrane potential-dependent K+ channel inhibitor, and we therefore suggest that acute alcohol administration led to CC relaxation through activation of K+ channels.
NO is important in the instantaneous relaxation of the cavernosal vessel and CC smooth muscle. NO is secreted as a result of eNOS activation in CC endothelial cells and by non-adrenergic, non-cholinergic neurotransmission at the cavernosal nerve terminal. NO activates guanylyl cyclase and increases the conversion of guanosine triphosphate transaminase to cGMP, which reduces intracellular Ca2+ through a complicated process and causes an erection by smooth muscle relaxation [1920]. In our study, the effect of alcohol on CC relaxation was not significantly inhibited by pretreatment with L-NAME, which is a NO synthesis inhibitor, or methylene blue, which is a guanylyl cyclase inhibitor. Therefore, we suggest that the CC relaxation effect was not related to the NO-cGMP pathway in acute alcohol administration.
The major nerve bundles involved in penile erections arise from the pelvic nerve, and the nerve bundles that inhibit penile erections originate from the sacral sympathetic nerve [21]. Therefore, electrical stimulation of the pelvic nerve and the cavernosal nerve leads to erection. In our study, the blood alcohol concentration peaked 2 hours after alcohol administration in vivo in rats, and the ICP/MAP percentage change due to the electric stimulation of the cavernosal nerve after acute alcohol administration was significantly higher in the 2-hour alcohol group than in the control group.
cAMP and cGMP are intracellular second messengers engaged in CC smooth muscle relaxation. They activate protein kinase A and protein kinase G, thereby activating K+ channels and inactivating Ca2+ channels, which prevents the intracellular infusion of Ca2+, moves the intracellular Ca2+ to the Golgi body, and causes relaxation of the CC smooth muscle [22]. In our study, cAMP significantly increased in the CC of the 2-hour alcohol group, which showed the most erections.
Therefore, the CC relaxation observed after acute alcohol administration was caused by the activation of β-receptors, cyclooxygenase, and K+ channels, and the 2-hour alcohol group had a significantly greater ICP/MAP percentage and intra-cellular cAMP concentration. We therefore propose that acute alcohol administration causes erections by activating the cAMP pathway.
Lizarte et al [23] performed an in vitro organ bath study using rats divided into a chronic 4-week alcohol (20%) group and a 4-week water group, and reported that these 2 groups did not show significant differences in CC smooth muscle tissue contraction depending on the PE concentration. Our study similarly did not show a significant difference between the 12-week alcohol group and the control group. Therefore, our results confirm that chronic alcohol administration does not significantly affect hemodynamic responses to autonomic nerve stimulation.
Elastic fibers, collagen fibers, and smooth muscle are known to play an important structural role in penile erections [242526]. Our study found that smooth muscle in the CC significantly decreased, while collagen fibers increased and became denser in the 12-week alcohol group, and that the measured collagen level was significantly higher in the 12-week alcohol group. Therefore, chronic alcohol administration may cause ED as a result of histological ultrastructure changes in the CC.
Our study found that that the eNOS expression regions were the same in both groups, but the response decreased in the 12-week alcohol group, and that eNOS expression was significantly lower in the 12-week alcohol group as determined by western blotting. Therefore, we suggest that chronic alcohol administration inhibits eNOS expression and can cause ED by reducing NO production.
Go to :
CONCLUSIONS
In conclusion, alcohol relaxes the CC in a dose-dependent manner via the activation of β-receptors, cyclooxygenase, and K+ channels. Acute alcohol administration activates the cAMP pathway and can have a positive effect on erectile function. Meanwhile, chronic alcohol administration changes the ultrastructures of the CC and suppresses eNOS expression, thereby leading to ED.
Go to :
 XML Download
XML Download