

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sexual health and well-being has a direct effect on overall quality of life (QoL) [12]. The prevalence of erectile dysfunction (ED), which can thus impact QoL, is increasing as the population ages [3]. ED is usually accompanied by benign prostatic hyperplasia (BPH) in elderly patients [4], and the pathophysiology of ED and BPH is very closely related [56]. Several recent studies have reported that medical therapy for ED or BPH could each influence the other [56]. From the surgeon's point of view, the idea that surgical treatment for BPH might affect ED is a focus of current research [78910111213].
Although many researchers have examined changes in erectile function after photoselective vaporization of the prostate (PVP), published findings are inconsistent [789101112]. For example, Paick et al [7] reported that sexual functioning improved after PVP, whereas Bruyère et al [8] concluded that erectile function after PVP did not improve or was similar to that before PVP. In contrast, Hossack and Woo [9] reported a significant decrease in erectile function after PVP.
These conflicting results might be due to variation in patient characteristics. For example, some of the studies included mainly patients with normal erectile function [9], whereas others involved mainly patients with underlying ED [78]. The analytic methods used to evaluate changes in erectile function also differed. Although most of the studies used the same questionnaire (i.e., the 5-item International Index of Erectile Function [IIEF-5]), they used different definitions of what constituted a significant change in erectile function [7891011121314]. Thus, based on the current literature, it is not possible to draw any conclusions about the impact of PVP on erectile function. Unlike the previous studies, we divided the patients into 5 groups according to their baseline IIEF-5 scores and evaluated the change in erectile function after treatment with a 120-W GreenLight high-performance system (HPS)-PVP.
MATERIALS AND METHODS
We retrospectively reviewed 493 consecutive patients who underwent HPS-PVP for symptomatic BPH at SMG-SNU Boramae Medical Center between January 2008 and December 2012.
A single surgeon (H.S.) performed all the HPS-PVP. Preoperatively, all the patients were asked to fill out an International Prostate Symptom Score (IPSS)/QoL questionnaire, which included questions about underlying diseases, such as diabetes mellitus and hypertension. Their IIEF-5 scores were also recorded. Laboratory tests including a test for prostate-specific antigen were performed, and the shape and size of the prostate were evaluated using transrectal ultrasonography. Uroflowmetry, including the post-void residual urine volume (PVR), was included in the routine preoperative checklists.
Perioperatively, the operative time, lazing time and total applied energy were recorded. Postoperative complications were reported and classified according to the Clavien-Dindo system. All the HPS-PVP patients visited the center at postoperative 1, 3, 6, 12, and 24 months. At each visit, their IPSS and IIEF-5 scores were recorded, and uroflowmetry with PVR was performed.
Patients with a previous history of BPH surgery or pelvic surgery were excluded from the analysis. Patients with other malignant diseases and neurogenic components were excluded. And patients with no sexual activity were also excluded. Ultimately, a total of 177 patients were included in this analysis. Their preoperative and perioperative findings were reviewed, and their postoperative 6-month, 1-year, and 2-year follow-up outcomes were retrospectively assessed.
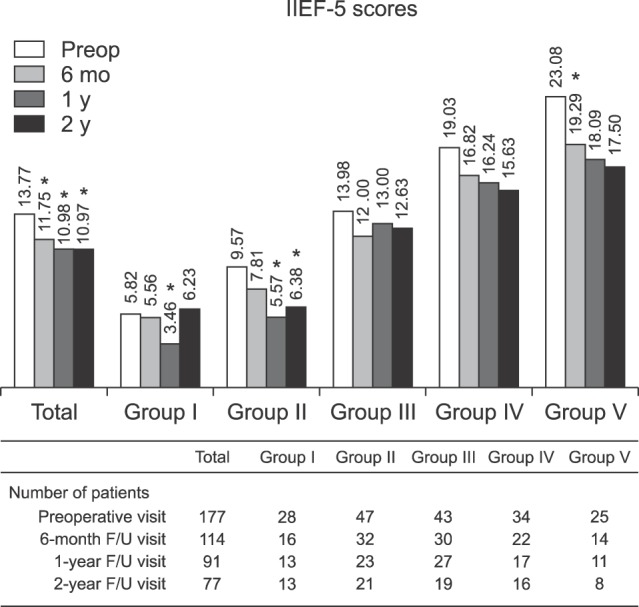
The patients were divided into 5 groups according to their preoperative IIEF-5 scores: Group I (IIEF-5: 5~7, severe erectile dysfunction, n=28), II (IIEF-5: 8~11, moderate erectile dysfunction, n=47), III (IIEF-5: 12~16, mild to moderate erectile dysfunction, n=43), IV (IIEF-5: 17~21, mild erectile dysfunction, n=34), and V (IIEF-5: 22~25, no erectile dysfunction, n=25). A meaningful change in postoperative erectile function was defined as more than a 5-point increase or decrease between the preoperative and postoperative 6-month IIEF-5 scores [9]. Based on this definition, we analyzed the preoperative risk factors for an increase or decrease in erectile function using a multivariate analysis.
1. Ethics statement
The study protocol was approved by the Institutional Review Board (IRB No. 26-2016-123) and the procedure in the present study complies with the Declaration of Helsinki (Edinburgh revision, 2000). Informed consent was waived by the IRB.
2. Statistical analysis
Statistically significant differences in the preoperative and postoperative parameters of the 5 subgroups were analyzed using one-way ANOVA and post hoc tests. To compare the pre- and postoperative clinical variables, an analysis of variance or a paired t-test and Wilcoxon's signed-rank test were used. To evaluate preoperative risk factors for a meaningful change in the IIEF-5 score, a logistic regression analysis was used. A p-value of <0.05 was considered statistically significant, and commercially available statistical software (IBM SPSS ver. 22.0; IBM Co., Armonk, NY, USA) was used to analyze the data.
RESULTS
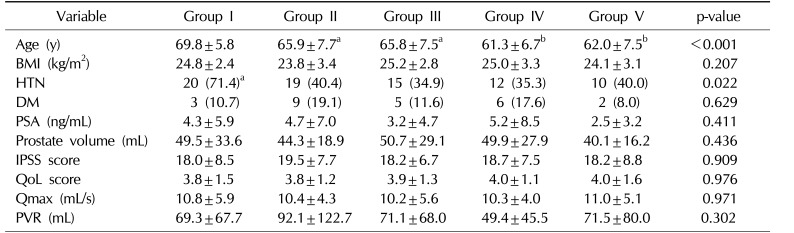
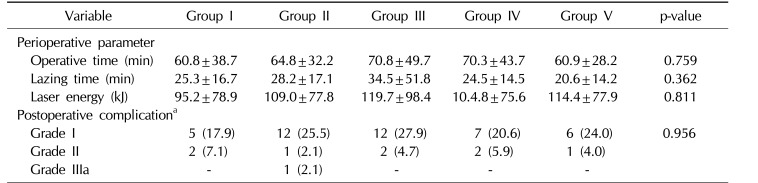
The preoperative clinical parameters of the 5 groups are summarized in Table 1. Among the parameters, the patient's age and presence of hypertension significantly differed in the 5 groups. Older age was associated with lower IIEF-5 scores. The presence of hypertension was higher in Group I than the other groups. Perioperative parameters, such as the operative time, applied energy, and postoperative complication rates showed no statistical differences (Table 2).
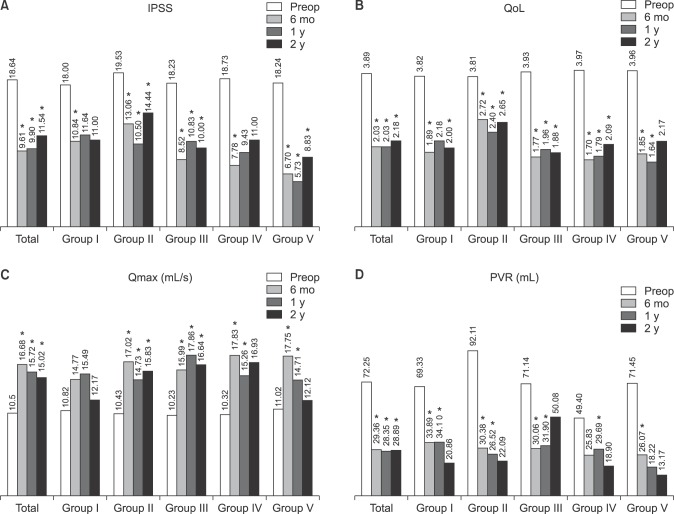
The postoperative follow-up rates at 6 months, 1 year, and 2 years were 64.4%, 51.4%, and 43.5%, respectively. After HPS-PVP, subjective and objective voiding parameters were significantly improved and sustained during the 2 years in all the groups (Fig. 1).
When we analyzed all the patients, there was a significant postoperative decline in their IIEF-5 scores. However, in the analysis of each group, the pattern of decrease varied among the groups. Group V showed the greatest deterioration of IIEF-5 after PVP (Fig. 2).
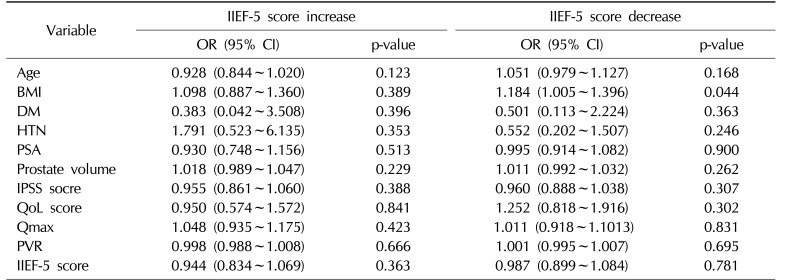
At postoperative 6 months, there were meaningful changes in the IIEF-5 scores of 55/114 patients (48.2%), with a postoperative increase in 18 cases (15.8%) and a decrease in 37 cases (32.5%). In the multivariate analysis of the preoperative clinical parameters, there was no significant risk factor associated with a postoperative increase in the IIEF-5 scores. On the other hand, body mass index (BMI) (odds ratio=1.184, p=0.044) was the only preoperative parameter associated with a meaningful decrease in the postoperative IIEF-5 scores after PVP (Table 3).
DISCUSSION
Recent studies have suggested that BPH is usually accompanied by ED [151617]. Despite the improvement in voiding symptoms after BPH surgery, the reported adverse impact of the surgery on erectile function is a major concern [4]. Generally, BPH surgery is irreversible. Thus, providing accurate and detailed information to patients about potential adverse effects of the surgical procedure is very important. Various surgical methods have been introduced and developed for symptomatic BPH, and the sexual impact of these methods has been investigated [181920].
Many researchers have studied changes in erectile function after PVP, but they have not reached a conclusion about the effect of PVP on erectile function [7891011121314]. As mentioned earlier, Paick et al [7] reported that sexual functioning improved after 6 months following treatment with 80-W potassium-titanyl-phosphate (KTP) PVP. Bruyère et al [8] prospectively analyzed the 2-year, long-term outcomes of 149 patients after KTP-PVP in 2010. They concluded that, in most cases, the erectile function after PVP was similar to that before PVP. In contrast, Hossack et al [9] reported that erectile function significantly decreased after HPS-PVP from the prospective study of 328 patients with a 1-year follow-up.
The main cause of these discrepancies is considered to be the variation among the study populations. The mean preoperative IIEF-5 scores were 11.3 in Paick's study, 8.0 in Bruyère's study, and 18.4 in Hossack's study [789]. We hypothesized that if the study were to include patients with severe preoperative ED, the postoperative effect of PVP on erectile function would be non-significant, whereas if the study population were composed of patients with normal erectile function, PVP would have a negative effect on erectile function.
In this hypothesis, the changes in erectile function after PVP might depend on the preoperative erectile function. Therefore, to evaluate the change in erectile function after PVP, we classified the patients into different groups according to their baseline IIEF-5 scores. Interestingly, our results showed that the erectile function declined in all the groups after HPS-PVP, with the most notable deterioration observed in patients with normal preoperative erectile function. On closer inspection after dividing the groups, the erectile function of preoperatively normal patients was significantly reduced function at the 6-month visit after PVP. Meanwhile, the previous ED patients did not show a significant change after the surgery.
Comparing the preoperative and postoperative 6-month IIEF-5 scores, 3 patients (10.7%) in group I, 5 patients (10.6%) in group II, 6 patients (14.0%) in group III, and 4 patients (11.8%) in group IV had an increase of more than 5 points in their IIEF-5 scores. There was no significant increase in the IIEF-5 scores in group V. On the other hand, there was a meaningful decrease in the IIEF-5 scores of 1 patient (3.6%) in group I, 15 patients (31.9%) in group II, 11 patients (25.6%) in group III, 7 patients (20.6%) in group IV, and 3 patients (12.0%) in group V. The pattern of change in erectile function varied according to the group (Table 1).
The effect of PVP on erectile function is still controversial. Thermal injury theory is one of the possible mechanisms to explain ED after PVP. Retrograde ejaculation after PVP could also be a cause of sexual dissatisfaction and lead to ED [821].
Voiding parameters were significantly improved and sustained at postoperative 2 years, but they were not associated with the preoperative IIEF-5 scores. Recent studies have shown that the pathophysiology of lower urinary infections that accompany BPH, and that of ED are similar. Therefore, medical treatments for BPH could affect ED and improve erectile function [56]. However, in the current study, the degree of improvement in voiding symptoms was not associated with a change in erectile function.
In the present study, we performed a multivariate analysis of the postoperative 6-month IIEF-5 scores to identify the risk factors associated with a change in erectile function. In the immediate postoperative period, a patient could experience discomfort, resulting in decreased sexual activity. Although it is impossible to evaluate the effect of surgery on erectile function, we judged that 6 postoperative months was enough time for a patient to recover from the temporary effects of the surgery and for normal sexual function to return. We used the postoperative 6-month IIEF-5 score as the main marker of the effect of the surgery and the 1- and 2-year follow-up IIEF-5 scores as markers of gradual progress after surgery. In the current study, patients with a higher BMI had a risk of decreased erectile function after the PVP. High BMI is one of the common risk factors for ED because metabolic syndrome, including obesity, could affect endothelial dysfunction of penile tissue and result in ED [22].
Urologists should inform patients about all possible complications after BPH surgery including deterioration of sexual function. Careful consultation and selection of appropriate patients for PVP is the first step. Reduction of applied energy during PVP and avoiding perioperative complications after PVP would also be helpful in preventing sexual dysfunction after PVP [2123].
Our study may be limited by its retrospective nature. To avoid selection bias, we applied strict exclusion and inclusion criteria. The initial review was performed with 177/493 (35.9%) of all consecutive patients. In the end, the final analysis included about 43.5% of the initial patients due to a lack of clinical information and follow-up loss. In addition, we did not assess other comorbidities, medications, and lifestyle factors, including diet and physical activity that could affect erectile function. However, this is the first study of changes in erectile function to take into account preoperative erectile function and to identify the potential preoperative risk factors that may be associated with a significant change in erectile function after PVP.
 XML Download
XML Download