

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
According to the International Continence Society criteria [1], nocturia is defined as the need to wake at night to void urine. Most people with severe nocturia, defined as waking 2 or more times per night to urinate, seek clinical treatment for the condition because it is associated with a reduction in health status and quality of life (QOL) [2345]. Waking at night to void causes lack of sleep and excessive daytime somnolence, reducing overall well-being, vitality, productivity, and mental health [23]. In particular, waking up to urinate 2 or more times per night is correlated with an increased risk of falling and limb/hip fractures [4]. Nocturia leads to increased mortality among elderly men, even after adjustment for possible contributory comorbidities and lifestyle factors [5]. Therefore, nocturia is a clinically significant condition.
Generally, nocturia becomes more common with age, and it is a characteristic clinical symptom of aging in the elderly [67]. Nocturia has a complex pathophysiology, and no direct cause has yet been identified. Various risk factors, such as aging, metabolic syndrome, hypertension, diabetes mellitus, congestive heart failure, sleep disorder, increased nocturnal urine volume, decreased bladder capacity, and benign prostate hypertrophy, have been suggested [8910]. In men, lower urinary tract symptoms (LUTS) occur concomitantly with an increase in prostate volume after 50 years of age. The incidence of LUTS increases with aging, with an overall prevalence of >50% in men aged >50 years, which exceeds the prevalence observed in elderly women [67].
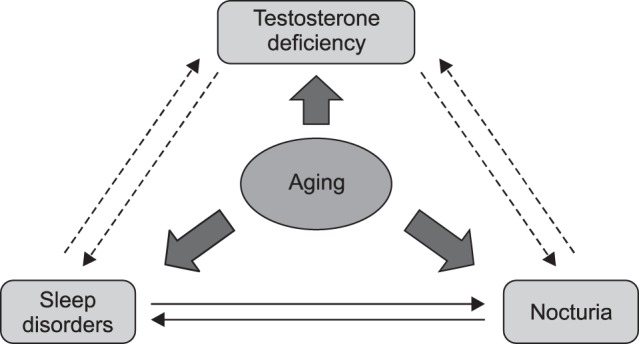
However, an alternative causative factor is closely associated with nocturia in elderly men. Serum testosterone levels gradually decrease in elderly men, and their reduction is associated with the symptoms of late-onset hypogonadism (LOH) syndrome [11]. LOH syndrome comprises a cluster of clinical symptoms, including decreased libido, muscle weakness, increased visceral fat, obesity, osteoporosis, anemia, and reduced insulin sensitivity [11121314]. Recent studies have demonstrated that testosterone deficiency is also linked with the development of LUTS [15], and that testosterone replacement therapy (TRT) can improve LUTS in hypogonadal men with benign prostatic hyperplasia (BPH) [1617]. In addition, testosterone levels are potentially correlated with circadian rhythms and sleep quality, which are perturbed by nocturia. Indeed, several studies have reported that testosterone deficiency has a negative effect on overall sleep quality that can be attenuated by TRT [181920]. These findings suggest that testosterone has direct and indirect correlations with the development of nocturia in elderly men (Fig. 1).
However, little is known about the correlation between testosterone and nocturia. Furthermore, there is a lack of compelling data on the efficacy of TRT for the management of nocturia in hypogonadal men. Therefore, in this article, we review the relationship between testosterone and nocturia, and the possible effects of TRT on nocturia in hypogonadal men.
RELATIONSHIP BETWEEN TESTOSTERONE AND NOCTURIA
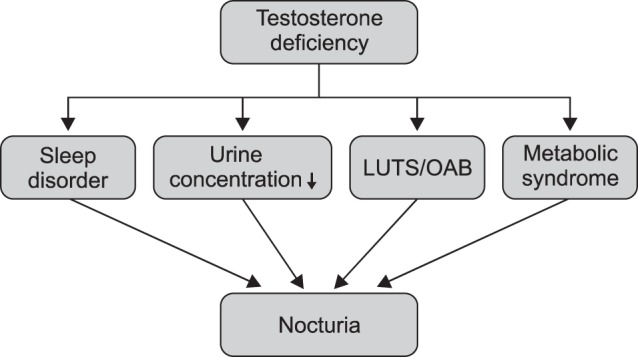
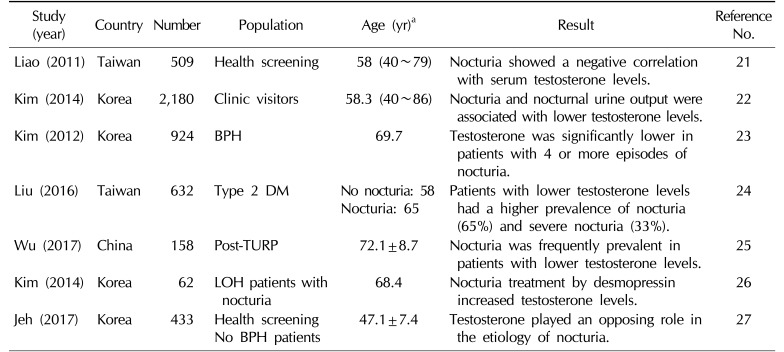
Many reports have investigated the relationship between testosterone and LUTS, whereas few have focused on the relationship between testosterone and nocturia in men [21222324252627]. Recent studies have suggested that testosterone has an ameliorative effect on nocturia (Table 1). Some of the benefits of TRT for nocturia can be explained by the effects of testosterone on sleep quality, urine-concentrating ability, metabolic syndrome, and LUTS/overactive bladder (OAB) (Fig. 2).
A cross-sectional study including 509 men aged 40 to 79 years found that serum testosterone levels were significantly associated with nocturia, and that men with serum testosterone levels in the upper quartile had a 44% lower risk of nocturia than men in the lowest quartile [21]. Another study involving 2,180 patients demonstrated that testosterone decreased 0.142 ng/mL for every time the patients woke at night to urinate, and that nocturia, especially nocturnal polyuria, was associated with decreased serum testosterone [22]. Kim et al [23] suggested that serum total testosterone levels may have a beneficial effect on lower urinary tract function, and showed that they were significantly lower in patients with 4 or more episodes of nocturia per night. In a cohort of 632 patients, patients with mean total testosterone levels of 2.21±0.51 ng/mL had a higher prevalence of nocturia [24]. Nocturia was also frequently observed among patients with lower testosterone levels who underwent transurethral prostate resection [25].
On the other hand, serum testosterone levels decrease significantly in men with nocturia, and low testosterone levels can be improved after 12 weeks of treatment with desmopressin [26]. Nocturia itself causes lack of sleep and decreases overall well-being, vitality, and mental health [23], which may contribute to a decrease in testosterone levels. Therefore, a negative feedback cycle can arise in hypogonadal men with nocturia, in which testosterone deficiency leads to the development of nocturia, and nocturia contributes to a decline in testosterone.
In contrast, another study suggested that men with higher serum testosterone levels may be at an increased risk of nocturia [27]. In 596 patients without BPH who were taking no medication for LUTS, nocturia showed a significant positive correlation with testosterone levels (odds ratio [OR]=1.15), suggesting that increased testosterone may contribute to the development of nocturia. However, the study population consisted of individuals who had relatively high testosterone levels (5.15±1.7 ng/mL) and were relatively young (47.1±7.4 years).
These conflicting data can be explained by differences among study populations and in the definitions of nocturia and LUTS, as well as by the influence of medications such as diuretics, anti-diabetic drugs, and alpha-1 blockers. Further studies are required for a more accurate understanding of the correlation between testosterone and nocturia.
1. Effects of testosterone on sleep quality
Sleep disorders are an established cause of nocturia [28], and testosterone is significantly associated with sleep quality and sleep disorders. Some categories of the Aging Males' Symptoms Scale, which is commonly used to screen for specific symptoms of LOH syndrome, include questions regarding sleep quality. Recent studies have demonstrated that endogenous testosterone production is dependent on the first 3 hours of uninterrupted deep sleep, and that various sleep disorders, including abnormal sleep quality and duration, circadian rhythm disruption, sleep apnea syndrome (SAS), and nocturia, can reduce testosterone levels [181929].
Testosterone deficiency can also affect sleep [30313233]. A cohort study involving 1,312 men aged 65 years and older demonstrated that those with lower testosterone levels had lower sleep efficiency, with more frequent nocturnal awakenings and less non-rapid eye movement (REM) sleep [30]. Another study found that healthy young men with high endogenous testosterone levels experienced greater subjective sleepiness and reduced cognitive function after 5 days of sleep restriction than those with low testosterone levels [18]. In mice, the lack of testosterone following gonadectomy reduces the quality and quantity of non-REM sleep, but this effect can be attenuated by TRT [31]. A recent randomized study found that 6 months of TRT could improve sleep conditions, QOL, and nocturia in hypogonadal men with a clinical diagnosis of nocturia [32]. Testosterone is likely to play a role in sleep. Low testosterone may affect overall sleep quality, but this may be counteracted by TRT. Improved sleep quality as a result of TRT may have a favorable effect on nocturia in hypogonadal men with nocturia.
However, supratherapeutic doses of exogenous testosterone, also known as testosterone abuse, are reportedly associated with reduced sleep duration, insomnia, and nocturnal awakenings [1833]. Furthermore, SAS is known to have a negative effect on sleep quality and testosterone levels. Although TRT is not recommended for hypogonadal men with untreated SAS, there is a lack of evidence regarding the adverse effects of exogenous testosterone on SAS [34].
2. Effects of testosterone on urine-concentrating ability
Testosterone is likely to be involved in the urine-concentrating ability of the kidneys. Nocturnal polyuria is considered the most significant contributory factor to nocturia. Indeed, a cross-sectional study including 2,180 patients with nocturia found that nocturnal polyuria was significantly associated with lower testosterone levels, and that individuals with low testosterone levels had greater nocturnal urine volume [22].
Several studies have demonstrated that testosterone plays a physiologic role in the maintenance of vasopressin levels and the urine-concentrating ability of the kidneys [35363738]. Experimental data have shown that, after orchiectomy, male rats exhibited decreased serum D-arginine-vasopressin and V2 vasopressin receptor expression, which reverted to normal with TRT [35]. The decreased number of vasopressin-binding sites in the kidneys of aging male rats has been found to be restored by TRT [36]. In addition, vasopressin is regulated by gonadal steroid hormones in the brain, with gonadectomy abolishing and TRT restoring normal vasopressin expression in adult men [37]. Furthermore, a clinical study investigating vasopressin levels via hypertonic saline infusions in hypogonadal men found that TRT improved the subnormal vasopressin response in aging men [38].
These studies suggest that loss of testosterone contributes to the development of nocturnal polyuria. However, little clinical evidence on the link between testosterone and polyuria is currently available, and further studies are required to reach a more definite conclusion.
3. Effects of testosterone on metabolic parameters
Metabolic factors, such as obesity, hypertension, and insulin resistance, are associated with testosterone deficiency [121314], and several of these factors are also associated with nocturia [8910]. After 11 years of follow-up, a long-term longitudinal study determined that men with lower total testosterone levels are at an increased risk of developing metabolic syndrome, with an OR of 2.3 (95% confidence interval, 1.5~3.4) [39]. In addition, recent studies have found TRT to be effective in improving various metabolic factors [121314].
In long-term studies, testosterone deficiency has been found to be associated with the development of various metabolic parameters, which may become causes of nocturia in elderly men with hypogonadism. Over the long term, TRT may improve nocturia indirectly by ameliorating various metabolic factors.
4. Effects of testosterone on lower urinary tract symptoms
Nocturia is prevalent among elderly men with BPH and LUTS, and has the most serious symptoms in elderly men. Recent studies have demonstrated that testosterone plays an important role in the development of LUTS and OAB in elderly men [15]. The reduced bladder capacity caused by BPH/LUTS and OAB in men is associated with nocturia.
Androgen receptors are found in the urothelium, including in the urinary bladder, prostate, and urethra. Testosterone modulates the autonomic nervous system and the activities of Rho-kinase, nitric oxide (NO) synthase, and phosphodiesterase-5 (PDE5) through these androgen receptors. Furthermore, testosterone activates endothelial NO synthase in the pelvis, consequently increasing NO concentration in the tissues of blood vessels, which may result in the dilation of pelvic vessels and alleviation of pelvic ischemia. Bladder blood flow is often decreased in patients with BPH and LUTS [40], and decreased bladder blood flow and ischemia caused by aging and arterial sclerosis are associated with the development of detrusor overactivity [4142]. Therefore, it may be possible to alter the interaction between testosterone and the urinary tract with NO, which may improve bladder neck relaxation, bladder capacity, and pelvic blood flow. Indeed, previous studies based on pressure-flow analysis and uroflowmetry have demonstrated that TRT for 1 year in hypogonadal men with LUTS effectively increased maximal bladder capacity and bladder compliance, and decreased detrusor pressure at maximal flow [1617].
Furthermore, recent clinical trials have reported that short-term TRT improved LUTS in hypogonadal men with BPH [324344454647]. However, limited information is available regarding the effects and safety of longer-term TRT in men with severe BPH and LUTS, and clinical reports on the effects of TRT on nocturia and OAB remain scarce. Further studies are required to reach more definitive conclusions.
REPORTED CLINICAL EFFECTS OF TESTOSTERONE REPLACEMENT THERAPY ON NOCTURIA
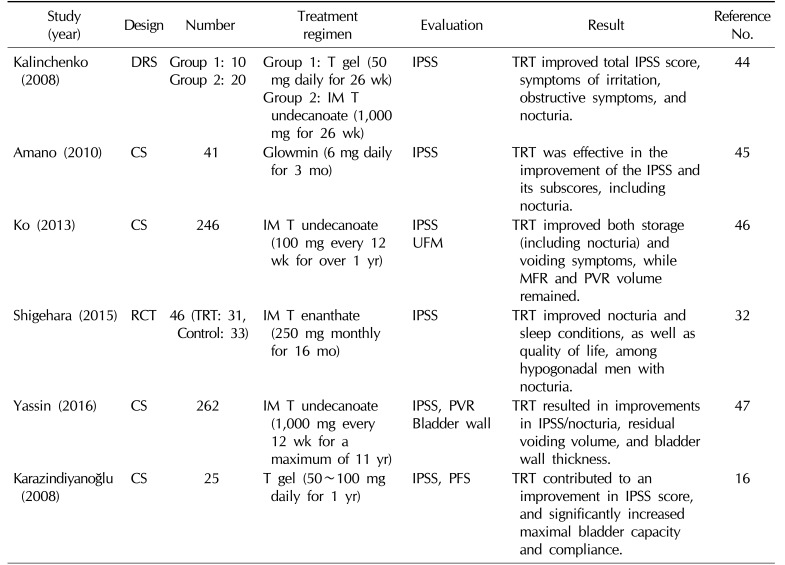
As described earlier, some clinical reports have asserted that TRT can improve LUTS in hypogonadal men with BPH, whereas the results of a very few studies have suggested that TRT may have a positive effect on nocturia (Table 2).
Kalinchenko et al [44] reported that 2 types of testosterone administration (testosterone gel or intramuscular testosterone undecanoate injection) for 26 weeks improved nocturia, total International Prostate Symptom Score (IPSS), symptoms of irritation, and obstructive symptoms in 30 hypogonadal men. In another case series study, application of testosterone ointment for 3 months by 41 patients with LOH syndrome improved LUTS and nocturia, achieving an increase in serum testosterone levels [45]. Moreover, TRT for over 1 year in patients with moderate LUTS receiving no medication for BPH improved both storage and voiding symptoms [46]. A recent sub-analysis of a randomized clinical trial examining the effects of TRT on LOH syndrome found that 6 months of TRT improved nocturia, sleep conditions, and QOL in hypogonadal men with nocturia [32]. Yassin et al [47] reported that TRT improved the IPSS score, nocturia, residual voiding volume, and bladder wall thickness, and that TRT interruption led these clinical conditions to worsen. Based on a pressure-flow study, TRT was found to contribute to a significant increase in prostate volume and an improvement in the IPSS score, and significantly increased maximal bladder capacity and compliance, which may improve storage symptoms, including nocturia [16].
However, there are some important limitations of these studies, in which nocturia was evaluated based on the scores for question 7 of the IPSS. This question is solely based on patients' subjective symptoms, and does not take into account a voiding diary or nocturnal urine volume. In addition, the safety and effects of TRT on urinary symptoms in patients with severe BPH or post-void residual urine volume have not yet been established. It is unclear whether the use of an alpha-1 blocker or PDE-5 inhibitor combined with testosterone is recommended in these patients. Further studies including patients with severe BPH/LUTS and the assessment of urine-concentrating disorders at nighttime with a voiding diary are required to understand the clinical effects of TRT on nocturia.
CONCLUSIONS
To improve QOL in patients with nocturia, their symptoms are generally addressed by restricting nighttime water intake and by treatment with medications, such as alpha 1-blockers, anticholinergic drugs, desmopressin, and drugs to induce sleep. However, a recent report demonstrated that nocturia treatment only reduced nocturnal voiding frequency, without improving QOL [5].
Various studies have suggested significant associations among nocturia, testosterone deficiency, LUTS/OAB, and sleep disorders. A negative feedback cycle can arise in hypogonadal men with nocturia, in which testosterone deficiency leads to the development of nocturia, and nocturia contributes to a decline in testosterone levels. Therefore, we should treat patients with nocturia appropriately to improve their QOL.
TRT is used worldwide as a treatment for many hypogonadal conditions, such as the loss of muscle mass and strength, reduced bone mineral density, sexual dysfunction, deterioration of insulin resistance, elevated visceral fat, and metabolic syndrome. As an additional benefit, TRT may also improve nocturia in hypogonadal men. However, limited information is currently available regarding the effects of TRT on nocturia in hypogonadal men, and further studies, including long-term observations of patients with varying severities of BPH or LUTS, are required to reach more definitive conclusions.
 XML Download
XML Download