

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radical prostatectomy (RP) is considered the gold-standard treatment for localized prostate cancer (PCa) according to most international clinical guidelines [12].
Despite several technical advances, the achievement of good postoperative functional outcomes is still considered a troublesome issue for both patients and urologists; indeed, data reported in both open RP (ORP) and robot-assisted RP (RARP) series have consistently shown the postoperative incidence of erectile dysfunction (ED) and urinary incontinence (UI) to range from 6% to 68% and 4% to 31%, respectively [34]. Both conditions have been thoroughly assessed in terms of risk factors, physiopathology, and postoperative management [56]; similarly, patients are routinely counselled regarding the risk of erectile function (EF) and urinary continence (UC) impairment associated with RP [567]. However, there is a series of other functional side effects that can occur after RP in addition to ED and UC, which as a whole are referred to as neglected side effects [89]. Indeed, data mainly from ORP series have shown impairments in sexual desire, orgasmic function (OF), and penile morphology after surgery [89]. Among these conditions, orgasmic dysfunctions (ODs) have been highlighted by several authors who have reported a non-negligible incidence of orgasm-associated incontinence (climacturia), orgasm-associated pain, and modifications of orgasmic sensations [89]. Nevertheless, the awareness of these functional sequelae among both patients and physicians is still insufficient.
This manuscript aimed to summarise the previously published evidence regarding OF alterations occurring after RP, in order to analyse the overall incidence and the potential management of these distressful conditions.
Go to : 
ORGASMIC FUNCTION: PHYSIOLOGY
Orgasm has been defined as an intense transient peak sensation of pleasure that alters one's state of consciousness and has been associated with physical changes [10]. An International Conference on Sexual Medicine Committee has stated that the experience of orgasm is a distinct cortical event, associated with the perception of striated muscle contractions and resulting in semen expelled during ejaculation, mediated through sensory neurons in the pelvic region [11]. Although it is considered to be a distinct physiological process, male orgasm is strictly related to the process of ejaculation (Fig. 1A) [10]. Ejaculation and orgasm are based on a complex interplay between the central nervous system and the peripheral nervous system, with the involvement of several neurotransmitters, including dopamine, norepinephrine, serotonin, acetylcholine, gamma-aminobutyric acid, and nitric oxide [12]; moreover, hormonal pathways may influence the process of ejaculation, with active roles played by oxytocin, prolactin, thyroid hormone, glucocorticoids, and sex hormones [1012].
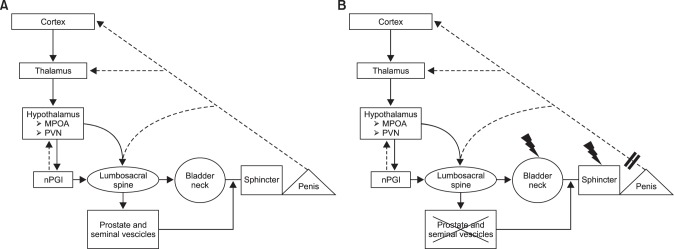
Studies assessing brain function during ejaculation and orgasm using positron emission tomography [13] have shown that certain areas become hyperactivated during these processes. The parvicellular part of the subparafascicular thalamus, the posterodorsal preoptic nucleus, and the posterodorsal medial amygdaloid nucleus are all involved, and have connections with the medial preoptic area (MPOA) of the hypothalamus, which has been found to play an extensive role in controlling sexual behaviour [10]. Moreover, the MPOA showed further connections to the paraventricular thalamic nucleus (PVN), the periaqueductal grey, and the paragigantocellularis nucleus (nPGI) [10]. The PVN is known to have projections to the pudendal motor neurons in the L5~L6 spinal segment and to autonomic neurons located into the lumbosacral spinal cord; overall, the MPOA has been shown to be involved in the stimulation of the ejaculatory response through interactions with the nPGI at the PVN [14].
At the peripheral level, the main sensory input comes from the dorsal nerve of the penis transmitting sensation from the genital area to the spinal cord [15]; this stimulation is potentiated by other areas at the level of the perineum and the testes.
The first step of the ejaculation process is the emission phase, characterized by closure of the bladder neck, preventing retrograde ejaculation, followed by the ejection of prostatic secretions and spermatozoa from the vas deferens into the prostatic urethra. Both the pelvic and the hypogastric plexus play a major role in the emission phase, involving mainly the sympathetic neurons; moreover, cerebral control over the spinal and peripheral neuronal elements is exerted in response to physical or visual stimulation [16]. Subsequently, the ejection of semen through the urethral meatus is known as the expulsion phase, and is characterized by contractions of the pelvic striated muscles, the bulbospongiosus and ischiocavernosus muscles [17]. Moreover, the bladder neck remains closed and the external urinary sphincter relaxes, and the pudendal nerve sensory stimuli resulting from the increased pressure in the posterior urethra and the contraction of the urethral bulb and other accessory sexual organs are processed at the level of the brain, thus inducing the sensation of orgasm [12].
Go to :
PHYSIOPATHOLOGY OF ORGASMIC DYSFUNCTIONS AFTER RADICAL PROSTATECTOMY
The surgical removal of the prostate along with the seminal vesicles and part of the vas deferens that occurs during RP has been associated with specific alterations of OF resulting from a disruption of the physiological process of orgasm/ejaculation at different levels (Fig. 1B).
Unpreventable damage to the bladder neck, and eventually to the sympathetic fibres responsible for bladder neck contraction and external sphincter relaxation during the expulsion phase of ejaculation, has been proposed as a possible mechanism responsible for orgasm-associated UI after RP (e.g., climacturia, which is defined as a leakage of urine occurring at orgasm) [9]. Moreover, in a single study aiming to assess the pathophysiologic mechanisms of climacturia, Manassero et al [18] analysed video-urodynamic data coming from a series of patients with post-RP orgasm-associated UI compared to a control group; they showed a significantly lower functional urethral length in patients with climacturia compared to controls, thus concluding that final urethral length may play a major role in determining this specific orgasmic alteration.
Similarly, a postulated theory regarding the occurrence of a muscle spasm or dystonia in the bladder neck and/or pelvic floor at the time of orgasm has been considered as the main explanation for reported post-RP painful orgasm (PO) episodes [19]. This theory has been proposed based on observations of patients with chronic pelvic pain syndrome experiencing exacerbation of their painful sensations during ejaculation/orgasm; in these patients, the administration of an alpha-lytic drug was associated with improved symptoms [19]. Similarly, these drugs have led to the partial improvement of orgasm-associated pain in patients treated with RP [19]. These theories have been corroborated by Mogorovich et al [20], who showed that in a cohort of 1,288 RP patients, a seminal vesicle-sparing technique was significantly associated with postoperative PO; indeed, the contraction of the residual seminal vesicle at the time of orgasm could be responsible for eliciting pain in these men, thus supporting other findings showing an improvement of symptoms with alpha-blockers, given their proven effect in decreasing seminal vesicle contraction [21].
Finally, disruption of the ejaculatory mechanism, resulting in postoperative anejaculation, has been associated with altered orgasmic sensations, defined as the inability to achieve an orgasm (anorgasmia) or a markedly diminished intensity of orgasmic sensations [22]. Numerous explanations for this have been proposed. From an organic standpoint, post-RP erectile difficulty could impair the stimulation of the dorsal penile nerve, thus reducing the afferent sensory stimuli responsible for orgasm/ejaculation [9]; moreover, postoperative anejaculation could greatly affect patients' psychological profile, creating a feeling of loss of masculinity, which in turn may affect orgasmic intensity [12]. In this context, in a study assessing OF in a cohort of 63 patients after RP, Messaoudi et al [23] showed that among the most sexually motivated patients, 76.0% reported loss of masculine identity, 52% reported loss of self-esteem, and 36.0% reported performance anxiety. Similarly, the psychological distress related to surgery and cancer diagnoses may have a negative impact on the patient's overall sexual health, including perceptions of orgasm [9].
Go to :
PREVALENCE OF ORGASMIC DYSFUNCTIONS AFTER RADICAL PROSTATECTOMY
Despite having been poorly studied in comparison with UI and ED, the occurrence of postoperative neglected sexual side effects has been reported in several studies that considered sexual desire, OF, and penile morphometric changes after RP [89]. In particular, the prevalence and predictors of climacturia, PO, and reduced orgasmic sensations/anorgasmia have been investigated.
1. Climacturia
The exact prevalence of climacturia in patients who undergo RP is unknown, given the huge variability in reported rates, ranging between 20% and 93% (Table 1) [232425262728293031]. In 1996, Koeman et al [24] first assessed orgasmic problems in a small series of patients treated with RP and reported that 9 out of 14 patients experienced involuntary loss of urine at orgasm. Similarly, Barnas et al [27] reported a rate of postoperative climacturia as high as 93%, although in 44% of the cases the event occurred rarely, while climacturia occurred at every orgasm in only 16% of patients. In a prospective survey including 42 patients, climacturia was reported in 45% of cases, with 58% of them complaining of losing only a few drops of urine, while 16% reported a loss of more than 1 ounce [25]. Interestingly, O'Neil et al [29] assessed sexually related side effects in a series of 412 patients treated with surgery and/or radiation therapy for PCa; these authors showed an overall rate of climacturia as high as 22.6% after treatment, with rates of 28.3%, 5.2%, and 28.6% after surgery, radiation, or both, respectively.
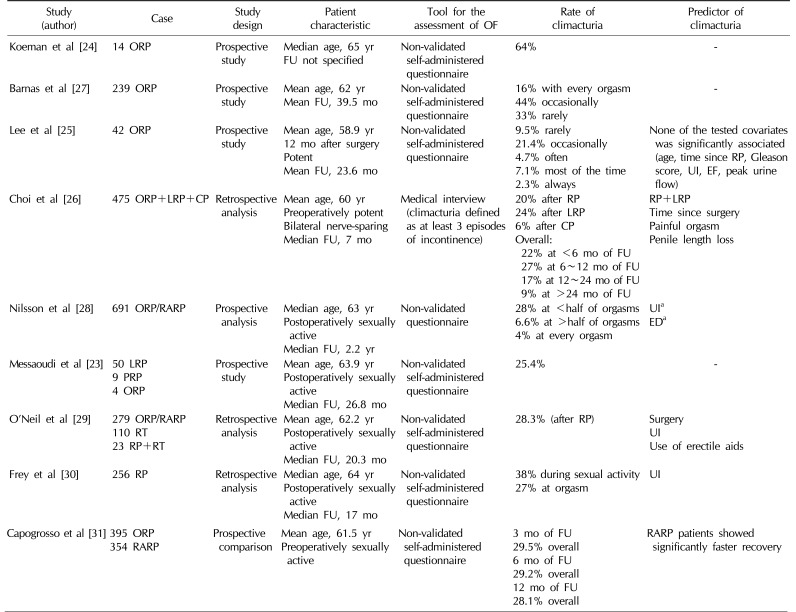
Table 1
Studies reporting the prevalence of climacturia after radical prostatectomy
| Study (author) | Case | Study design | Patient characteristic | Tool for the assessment of OF | Rate of climacturia | Predictor of climacturia |
|---|---|---|---|---|---|---|
| Koeman et al [24] | 14 ORP | Prospective study |
Median age, 65 yr FU not specified |
Non-validated self-administered questionnaire | 64% | - |
| Barnas et al [27] | 239 ORP | Prospective study |
Mean age, 62 yr Mean FU, 39.5 mo |
Non-validated self-administered questionnaire |
16% with every orgasm 44% occasionally 33% rarely |
- |
| Lee et al [25] | 42 ORP | Prospective study |
Mean age, 58.9 yr 12 mo after surgery Potent Mean FU, 23.6 mo |
Non-validated self-administered questionnaire |
9.5% rarely 21.4% occasionally 4.7% often 7.1% most of the time 2.3% always |
None of the tested covariates was significantly associated (age, time since RP, Gleason score, UI, EF, peak urine flow) |
| Choi et al [26] | 475 ORP+LRP+CP | Retrospective analysis |
Mean age, 60 yr Preoperatively potent Bilateral nerve-sparing Median FU, 7 mo |
Medical interview (climacturia defined as at least 3 episodes of incontinence) |
20% after RP 24% after LRP 6% after CP Overall: 22% at <6 mo of FU 27% at 6~12 mo of FU 17% at 12~24 mo of FU 9% at >24 mo of FU |
RP+LRP Time since surgery Painful orgasm Penile length loss |
| Nilsson et al [28] | 691 ORP/RARP | Prospective analysis |
Median age, 63 yr Postoperatively sexually active Median FU, 2.2 yr |
Non-validated questionnaire |
28% at <half of orgasms 6.6% at >half of orgasms 4% at every orgasm |
UIa EDa |
| Messaoudi et al [23] |
50 LRP 9 PRP 4 ORP |
Prospective study |
Mean age, 63.9 yr Postoperatively sexually active Median FU, 26.8 mo |
Non-validated self-administered questionnaire | 25.4% | - |
| O’Neil et al [29] |
279 ORP/RARP 110 RT 23 RP+RT |
Retrospective analysis |
Mean age, 62.2 yr Postoperatively sexually active Median FU, 20.3 mo |
Non-validated self-administered questionnaire | 28.3% (after RP) |
Surgery UI Use of erectile aids |
| Frey et al [30] | 256 RP | Retrospective analysis |
Median age, 64 yr Postoperatively sexually active Median FU, 17 mo |
Non-validated self-administered questionnaire | Non-validated self-administered questionnaire | UI |
| Capogrosso et al [31] |
395 ORP 354 RARP |
Prospective comparison |
Mean age, 61.5 yr Preoperatively sexually active |
Non-validated self-administered questionnaire |
3 mo of FU 29.5% overall 6 mo of FU 29.2% overall 12 mo of FU 28.1% overall |
RARP patients showed significantly faster recovery |
OF: orgasmic function, ORP: open radical prostatectomy, LRP: laparoscopic radical prostatectomy, CP: cystoprostatectomy, RARP: robot-assisted radical prostatectomy, PRP: perineal radical prostatectomy, RT: radiotherapy, RP: radical prostatectomy, FU: follow-up, UI: urinary incontinence, ED: erectile dysfunction.
aUnivariate analysis.
![]()
More recently, Frey et al [30] reported a similar rate of 38% of patients complaining of UI associated with sexual activity in a series of 256 patients following RP; moreover, these authors asked patients to objectively quantify how much this issue negatively impacted their sexual activity, and reported a median “bother” score of 3 out of 10, which still seems surprisingly low. Conversely, in other series, climacturia was found to severely impact various aspects of sexual life, including low partner satisfaction, fear of intercourse failure, and low satisfaction with orgasm [28].
The rates of climacturia after minimally invasive surgery have been also assessed. Choi et al [26] previously showed a 20% rate of climacturia after ORP compared to a 24% rate after laparoscopic RP. In the same survey, the authors investigated the prevalence of climacturia at different times after surgery, showing a decrease in prevalence from 27% after 6 to 12 months to 9% after more than 24 months post-RP. Similar results supporting the possibility of recovering from climacturia were also reported by Blaivas [32] . More recently, in a series of 354 RARP patients, climacturia was reported by 31.1% of patients at a 1-year postoperative follow-up assessment, with no significant difference compared to an age-matched ORP group [31]. Overall, fewer than 1% of patients complaining of climacturia had recovered from their complaint by 12 months after surgery, and 84% of them still had not recovered from climacturia after 60 months. However, after adjusting the analyses for the type of surgery, the authors observed that patients treated with RARP showed significantly higher rates of recovery from climacturia than the ORP group, with a rate of recovery of 8% and 5% after RARP and ORP at a 24-month assessment, respectively; likewise, the rates of recovery were 48% and 13% after the 2 types of surgery after more than 80 months, respectively [31].
UI has been previously associated with the occurrence of climacturia after surgery [282930]. Indeed, in an assessment of the potential predictors of climacturia, Frey et al [30] showed a higher risk of climacturia in patients with postoperative UI, and similar findings were observed by O'Neil et al [29] in patients treated with surgery or radiation therapy. Conversely, Nilsson et al [28] explored orgasm-associated incontinence in a consecutive series of 691 sexually active RP patients, of whom 268 reported climacturia despite recovering full UC in 86% of cases. Of note, all these studies investigated the prevalence of climacturia after surgery in a non-time-dependent fashion; in contrast, when looking at potential predictors of recovery from climacturia over time, robotic surgery emerged as the only independent predictor of recovery, after adjusting for age at surgery, body mass index, and nerve-sparing status, as well as UC and EF recovery rates [31].
2. Painful orgasm
Orgasm-associated pain is defined as a painful sensation occurring at the time of orgasm, which has been mainly reported at the level of the penis but can potentially occur at a number of other sites [27]. Previous data have reported rates of up to 19% of patients complaining of PO after RP (Table 2) [2024272830313334]. More recently, Frey et al [30] reported that 23 out of 256 patients treated with RP suffered from PO over the postoperative period. In general, painful sensations have been reported at the level of the penis, the rectum, or the lower abdomen [27]. In a series of 702 RP patients, Matsushita et al [33] reported a 12% rate of PO, with the most common location of pain being on the penile shaft (70%) or in the testes (22%). Barnas et al [27] showed that 33% of those suffering from post-RP PO experienced pain every time they engaged in intercourse. Capogrosso et al [31] assessed PO rates in a series of 395 ORP cases compared to 354 RARP cases, showing a comparable overall rate of self-reported PO of 9.5%. Interestingly, recovery rates of 10% and 30% from PO were observed at 12 and 60 months after surgery, respectively, thus corroborating previous findings that demonstrated a decrease in the frequency and intensity of pain throughout the follow-up [33]. Although UI and EF impairment have been previously associated with orgasmic modifications after surgery [25293035], no data have suggested strong predictors for PO occurrence after RP; however, a significantly higher prevalence of PO after ORP than after RARP has been reported (9.5% vs. 11.6%; p=0.04) [31]. Similarly, in a series of 156 RARP cases, Tewari et al [34] reported that only 3.2% of patients complained of PO after treatment. Overall, these data seem to suggest that robotic surgery may have a protective effect in terms of the incidence of PO, possibly related to the more careful and precise dissection of the bladder neck during RARP than in the open approach [31]. However, when included in a multivariable model, RARP was not confirmed as an independent predictor of the low incidence of PO [31]. Conversely, Mogorovich et al [20] analysed the impact of different surgical techniques on postoperative orgasmic modifications in a series of 1,411 RP cases; they found that the seminal vesicle-sparing technique was significantly associated with a higher rate of postoperative PO, with a relative risk of 2.33 (95% confidence interval, 1.0~5.3), while the nerve-sparing and bladder neck-sparing techniques were not.
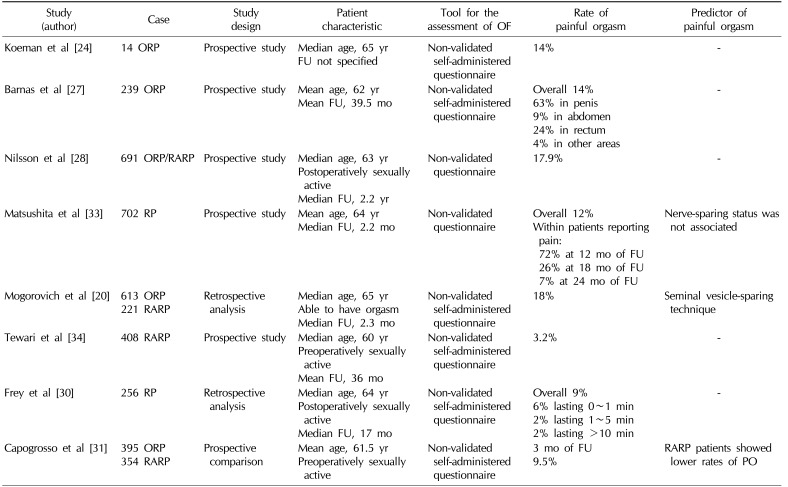
Table 2
Studies reporting the prevalence of painful orgasm after radical prostatectomy
| Study (author) | Case | Study design | Patient characteristic | Tool for the assessment of OF | Rate of painful orgasm | Predictor of painful orgasm |
|---|---|---|---|---|---|---|
| Koeman et al [24] | 14 ORP | Prospective study |
Median age, 65 yr FU not specified |
Non-validated self-administered questionnaire | 14% | - |
| Barnas et al [27] | 239 ORP | Prospective study |
Mean age, 62 yr Mean FU, 39.5 mo |
Non-validated self-administered questionnaire |
Overall 14% 63% in penis 9% in abdomen 24% in rectum 4% in other areas |
- |
| Nilsson et al [28] | 691 ORP/RARP | Prospective study |
Median age, 63 yr Postoperatively sexually active Median FU, 2.2 yr |
Non-validated questionnaire | 17.9% | - |
| Matsushita et al [33] | 702 RP | Prospective study |
Mean age, 64 yr Median FU, 2.2 mo |
Non-validated questionnaire |
Overall 12% Within patients reporting pain: 72% at 12 mo of FU 26% at 18 mo of FU 7% at 24 mo of FU |
Nerve-sparing status was not associated |
| Mogorovich et al [20] |
613 ORP 221 RARP |
Retrospective analysis |
Median age, 65 yr Able to have orgasm Median FU, 2.3 mo |
Non-validated self-administered questionnaire | 18% | Seminal vesicle-sparing technique |
| Tewari et al [34] | 408 RARP | Prospective study |
Median age, 60 yr Preoperatively sexually active Mean FU, 36 mo |
Non-validated self-administered questionnaire | 3.20% | - |
| Frey et al [30] | 256 RP | Retrospective analysis |
Median age, 64 yr Postoperatively sexually active Median FU, 17 mo |
Non-validated self-administered questionnaire |
Overall 9% 6% lasting 0~1 min 2% lasting 1~5 min 2% lasting >10 min |
- |
| Capogrosso et al [31] |
395 ORP 354 RARP |
Prospective comparison |
Mean age, 61.5 yr Preoperatively sexually active |
Non-validated self-administered questionnaire |
3 mo of FU 9.5% |
RARP patients showed lower rates of PO |
![]()
3. Alterations of orgasmic sensation
Overall, impaired orgasmic sensation has been reported in 33% to 77% of patients after RP [232427303435363738] (Table 3). In 1996, Helgason et al [36] observed a reduction in orgasmic pleasure in up to 70% of a small cohort of patients treated with RP. Subsequently, in a study specifically aimed to assess postoperative OF, 37% of 239 patients reported a decreased orgasm intensity, while a further 37% suffered from anorgasmia after RP [27]. Similarly, a complete postoperative absence of orgasm was observed in 20% of cases in a larger cohort of 671 patients after RP [37]. An even higher rate of 77.8% was reported by Messaoudi et al [23], who considered both anorgasmia and a decrease of orgasmic sensation. More recently, Frey et al [30] showed that in a cohort of 256 sexually active patients after RP, only 29% reported no change in terms of OF, while 60% experienced decreased orgasmic intensity; moreover, 146 patients (57%) complained of an increased time to reach orgasm compared to their preoperative status. Interestingly, Salonia et al [35] evaluated OF over time using the validated International Index of Erectile Function questionnaire (IIEF); although the evaluation was somewhat arbitrary because of the incomplete adequacy of the method for the study of a population that had formally lost ejaculation, the authors assessed the OF domain score (IIEF-OF) and showed a progressive OF amelioration throughout a 48-month postoperative period (F=4.02; p=0.007). Moreover, after adjusting for patients' age, EF, rate of UI, and the use of any pro-erectile drug, OF linearly increased with the postoperative improvement of EF at any single follow-up assessment (hazard ratio [HR]=0.425, p=0.015; HR=0.454, p<0.001; and HR=0.454, p<0.001 at 12-, 24-, and 36-month follow-ups, respectively). Finally, the OF score linearly decreased with age [35]. Similar findings were observed by Dubbelman et al [38], who showed in their cohort that OF was preserved in 77% of men younger than 60 years of age, but in only 61% of those older than 60 years (p<0.0001). Moreover, in an evaluation of the potential predictors of OF decrease, they found that patients treated with a nerve-sparing procedure were more likely to have normal OF after RP in a multivariable analysis (odds ratio=0.454; p=0.001); similarly, severe UI was significantly associated with postoperative orgasmic alterations (p=0.021). These findings were further confirmed by Hollenbeck et al [37], who showed that a nerve-sparing technique, younger age, and a prostate weight lower than 59 g were significantly associated with better OF outcomes after surgery. Overall, these data clearly underscore the direct link between EF and OF after RP, thus suggesting that factors influencing the recovery of normal EF after surgery, such as the patient's baseline characteristics and the surgical technique, could play a major role in influencing postoperative orgasm. Of note, Tewari et al [34] reported follow-up data of 408 patients treated with RARP, and showed that in men younger than 60 years of age and in those receiving bilateral nerve-sparing surgery, postoperative orgasm and potency were present in 92.9% and 90.5% of cases, respectively.

Table 3
Studies reporting the prevalence of altered orgasmic sensation after radical prostatectomy
| Study (author) | Case | Study design | Patient characteristic | Tool for the assessment of OF | Rate of altered orgasmic sensation | Predictor of altered orgasmic sensation |
|---|---|---|---|---|---|---|
| Koeman et al [24] | 14 ORP | Prospective study |
Median age, 65 yr FU not specified |
Non-validated self-administered questionnaire | 50% weakened orgasm | - |
| Helgason et al [36] | 342 PCa patients (22 RP) | Prospective study | Median age, 72 yr | Non-validated self-administered questionnaire | 14/20 (70.0%) decreased orgasmic pleasure | - |
| Hollenbeck et al [37] | 671 ORP | Retrospective analysis | FU of 4~52 mo | Expanded Prostate Cancer Index Composite questionnaire |
Anorgasmia in patients aged <58 yr 16% after BNS-RP 32% after UNS-RP 33% after NNS-RP |
Age Nerve-sparing Prostate weight <59 g |
| Barnas et al [27] | 239 ORP | Prospective study |
Mean age, 62 yr Mean FU, 39.5 mo |
Non-validated self-administered questionnaire |
37% anorgasmia 37% decreased orgasmic pleasure |
- |
| Dubbelman et al [38] | 458 ORP | Prospective study | Mean age, 63 yr | Non-validated self-administered questionnaire | 33.2% impaired orgasmic function |
Age Nerve-sparing |
| Salonia et al [35] | 334 ORP | Retrospective analysis |
Mean age, 61.8 yr Preoperatively sexually active Bilateral nerve-sparing |
International Index of Erectile Function questionnaire | International Index of Erectile Function: OF score linearly increased through follow-up |
Age International Index of Erectile Function: Erectile Function domain score |
| Tewari et al [34] | 408 RARP | Prospective study |
Median age, 60 yr Preoperatively sexually active Mean FU, 36 mo |
Non-validated self-administered questionnaire |
Rates of anorgasmia: BNS: 9.3% UNS: 17.9% NNS: 39.2% |
Age Nerve-sparing |
| Messaoudi et al [23] |
50 LRP 9 PRP 4 RARP |
Prospective study |
Mean age, 63.9 yr Postoperatively sexually active Median FU, 26.8 mo |
Non-validated self-administered questionnaire |
77.8% decreased orgasmic pleasure 39.7% anorgasmia |
- |
| Frey et al [30] | 256 RP | Retrospective analysis |
Median age, 64 yr Postoperatively sexually active Median FU, 17 mo |
Non-validated self-administered questionnaire |
60% decreased orgasm intensity 5% anorgasmia |
UI |
OF: orgasmic function, ORP: open radical prostatectomy, PCa: prostate cancer, RP: radical prostatectomy, RARP: robot-assisted radical prostatectomy, LRP: laparoscopic radical prostatectomy, PRP: perineal radical prostatectomy, FU: follow-up, BNS: bilateral nerve-sparing, UNS: unilateral nerve-sparing, NNS: non-nerve-sparing, UI: urinary incontinence.
![]()
Go to :
HOW TO MANAGE POSTOPERATIVE ORGASMIC DYSFUNCTIONS
Data regarding the available therapeutic tools to manage ODs occurring after RP are still scarce, for 2 main reasons: first, the overall assessment of these conditions by physicians in real-life settings is significantly less common than for other post-RP functional impairments (e.g., UI and ED); second, the physiopathology underlying ODs is far from being comprehensively elucidated.
Post-RP conservative management strategies for climacturia have never been tested with a proper scientific methodology; however, in a study enrolling 42 patients, of whom 45% complained of climacturia 2 years after surgery, Lee et al [25] reported that patients employed a range of coping mechanisms aimed at overcoming this issue, showing that 74% of them emptied their bladder before sexual activity, 11% used a condom, and 16% of patients avoided all sexual intercourse. Although the efficacy of these strategies has never been scientifically tested, based on the data regarding the amount of leakage occurring at orgasm in patients suffering from climacturia, it seems reasonable that those conservative strategies could be successfully applied; in this context, the self-reported volume of urine leakage associated with orgasm was ≤5 mL in 85.2% of cases in a recently published large series [31].
In a study aiming to determine the effect of pelvic floor muscle training (PFMT) on EF recovery after RP, Geraerts et al [39] assessed the impact of this strategy in terms of OF improvement and recovery from climacturia. After 3 months of treatment, 6 out of 9 patients reporting climacturia in the treatment group showed an improvement, as compared to no improvement in the untreated group (p=0.004), although the IIEF-OF domain scores did not significantly change after treatment. Overall, this sample appears too small to draw a final conclusion regarding the impact of PFMT on OF recovery after surgery. A different conservative strategy has been proposed by Mehta et al [40]; in a prospective study of 124 patients with climacturia, every patient was instructed to apply a penile tension loop during sexual stimulation, once they had achieved their highest-quality erection. At a 3-month follow-up evaluation, patients reported a significant decrease in terms of both the frequency of climacturia and the degree of leakage (p<0.01), with almost half of them reporting no climacturia at follow-up [40]. However, the lack of a control group and the absence of any multivariable analysis adjusting for potential confounders, such as EF improvement (which would account for patients receiving either phosphodiesterase type 5 inhibitors or intracavernous therapy) undermine the value of their findings.
Finally, climacturia has been assessed in the context of the outcomes of the surgical treatment of UI; a small cohort of 11 patients, sexually active after RP, was treated with either implantation of an artificial urinary sphincter (AUS) or an urethral sling (US) [41]. The authors showed a self-reported “marked” improvement of climacturia in 4 out of 4 patients treated with AUS and in 7 out of 7 men treated with US. In addition to the very small number of patients included, it must be noted that all the patients were also affected by UI, with a mean number of pads used per day of 6.4 and 3.8 for the AUS and US groups, respectively; in this context, one cannot be sure of the effect of these procedures in patients experiencing leakage only at the time of orgasm or during arousal.
Regarding possible strategies for managing patients complaining of PO after surgery, the only available evidence comes from a prospective non-placebo-controlled study including 98 patients reporting orgasm-associated pain, of whom 35% and 16% had been treated with RP and radiation therapy for PCa, respectively [19]. All patients received 0.4 mg/day of tamsulosin for 4 weeks; a significant decrease was found in the visual analogue scale (VAS) for pain assessment, with a drop of 2.7 points from before to after treatment. Of note, patients previously treated with RP had higher VAS scores at baseline and reported significant improvements after treatment. The main limitation of that study is the lack of a control group, meaning that it is impossible to rule out the possibility of a spontaneous recovery from PO unrelated to tamsulosin, as has been observed in other studies [19].
As for PO, the available therapeutic options for impaired or absent orgasmic sensation after surgery have been under-investigated. From a general perspective, there are no highly effective pharmacotherapies for altered orgasmic sensations, and the treatment is largely based on addressing potential causative factors, as well as on the use of psychotherapy [42]. Interestingly, Hollander et al [43] recently reported data from 131 patients with ODs treated with cabergoline, a dopamine agonist; the data showed that 66.4% of patients reported a subjective improvement in terms of orgasm. Of note, 17.6% of patients had undergone RP before cabergoline treatment, and in a multivariable analysis, a history of RP did not influence treatment outcomes. The only study specifically assessing the outcomes of treatment of orgasmic alterations in the post-RP setting was conducted by Nehra et al [44]. The authors developed a randomized, placebo-controlled study including 440 patients who underwent nerve-sparing RP and received either placebo or 10 mg or 20 mg of on-demand vardenafil no more than once per day. Their results showed that both drug doses significantly improved the OF domain of the IIEF questionnaire in comparison with baseline, with a mean increase of 4.4 to 5.9 after 12 weeks of treatment. It must be pointed out that the majority of the patients included had good preoperative characteristics in terms of baseline EF, comorbidities, and age; moreover, the IIEF questionnaire has never been validated as an in strument to assess decreased orgasmic sensation or anorgasmia. However, it is reasonable to believe that the improvement of EF due to vardenafil treatment could have a significant positive impact on overall sexual function, including OF.
Go to :
CONCLUSIONS
The assessment of the so-called neglected side effects after RP, including ODs, is still far from becoming part of common clinical practice related to the postoperative work-up of patients [45]. However, the overall prevalence of ODs after RP is not negligible; indeed, synthesizing the available data about the prevalence of altered orgasmic sensations, climacturia, and orgasm-associated pain, we should expect that patients treated with RP will complain of different forms of ODs in between 20% and 90% of cases. In this context, although the UC and EF outcomes data come from several well-conducted studies that used internationally-validated tools, no orgasm-specific questionnaires suitable for objectively assessing post-RP OF alterations are available. Therefore, almost all the data discussed in this review were collected using non-validated tools, thus potentially creating biases regarding the validity and generalizability of the findings. For the first time, Dubray et al [46] recently validated a brief self-report measurement of orgasm, assessing bodily and physiologic sensations perceived during climax; they developed a 22-item questionnaire analysing extragenital and genital sensations, spasms, nociceptive sensations, and sweating responses. Studies using this novel validated tool for the evaluation of post-RP OF are currently awaited.
A further major scientific gap in the context of ODs is related to the pathophysiology of these phenomena. Very few studies have aimed to identify the pathogenic mechanisms behind postoperative ODs, although it is certainly true that the overall modifications of the anatomy occurring at the level of the urogenital tract must be considered as a general and common pathologic substrate. However, as opposed to ED, we are currently not able to clearly identify potential predictors of post-RP ODs; indeed, within the different steps of the clinical management of patients who are candidates for RP, age is the only factor that would be useful to estimate preoperatively the risk of altered OF after surgery. Similarly, from a surgical standpoint, data supporting a role of either the nerve-sparing or bladder-neck-sparing technique in reducing the risk of occurrence of postoperative OF impairment are scarce. Lastly, no data have been published yet regarding possible strategies to enhance the recovery of normal OF in the immediate postoperative setting. However, given the significant link between EF and OF, we may speculate that all the factors that have been significantly associated with the risk of ED [5831] (and UI in the case of climacturia) may also play a major role in influencing OF outcomes after RP. This appears to be the case, although OF can still be normal after RP despite the absence of an erection [38].
Likewise, we are currently unable to offer proper treatment to patients complaining of ODs after surgery; indeed, although conservative strategies with potential good results could be suggested for climacturia and encouraging results have been published regarding the effect of UI surgery on the improvement of orgasm-associated incontinence, we are still far from being able to suggest satisfactory treatments for either PO or postoperative anorgasmia.
Overall, physicians should be aware of the risk of post-RP ODs in order to properly counsel every patient before a surgical treatment of any type; indeed, it has been previously shown that almost half of the candidates for RP were completely unaware of the occurrence of postoperative anejaculation [47]. Therefore, RP patients should be provided with realistic expectations regarding possible changes in their sexual life and well-being after surgery.
Go to :
 XML Download
XML Download