

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent years, individuals seeking medical services have developed a higher level of expectation of the healthcare service and more opportunities to access abundant information on medical knowledge or legal remedy. Medical consumers have taken various actions against hospitals such as filing lawsuits since medical disputes related to healthcare services have gone far beyond simple dissatisfaction. Under these circumstances, medical disputes related to medical malpractice have also increased along with the awareness of consumers' rights, access to information on medical technology, patient expectations, expectations for monetary compensation, and other factors. In South Korea (hereafter Korea), the number of medical disputes that have progressed to medical lawsuits has increased with the increased execution of medical malpractice legal remedies and acts on dispute mediation [1]. Furthermore, this increased number of medical lawsuits is likely due to an increase in the number of lawyers, expanded legal services in medical malpractice law firms, and the increased success rate for medical lawsuits (60%~70%). According to the Judicial Yearbook, the number of medical lawsuits filed in 1992 (n=82) increased by 10 times to 882 cases in 2002. Moreover, the frequency of medical disputes have almost doubled over the last decade from 1,674 cases in 2000 to 3,618 cases in 2010 in Korea (Fig. 1) [2].
To understand the progressive changes to the legal conditions in medical and hospital management environments in Korea, the present study was performed to minimize legal risk by resolving hardware and software problems associated with the medical environment. We analyzed lawsuit cases filed due to medical disputes throughout the last 13 years at Pusan National University Hospital (PNUH), which is located in the second large city in Korea, in hopes of maximizing the effectiveness of the hospital management services in PNUH.
MATERIALS AND METHODS
This study retrospectively reviewed and analyzed 55 closed lawsuit cases among the 64 civil medical lawsuits carried out at PNUH from January 2000 to April 2013 using medical records, petitions, briefs, and data from the Medical Dispute Mediation Committee. The reasons the lawsuits were filed, leading causes of death, court decision at the hearing phases, time period from the medical malpractice incident to legal proceedings, the duration of the hearing, final disposition, and amount of compensation claimed and decided (by year, motives and causes, leading causes of death, and medical departments) were collected from each of the closed cases. Statistical analyses were performed using SPSS for Windows ver. 15.0 (SPSS Inc., Chicago, IL, USA). For all analyses, t-tests were used. p values less than 0.05 were considered to indicate statistical significance. This study protocol was approved by the Institutional Review Board of PNUH. Because this study used publically accessible, de-identified data, the Institutional Review Board waived the requirement of informed consent.
RESULTS
1. Annual case distribution
The number of filed lawsuit cases ranged from a minimum of two to a maximum of 11 per year among the 55 civil lawsuits. The average annual number of lawsuit cases was 4.2. After 2010, the number of filed cases tended to decrease, but no statistically significant differences were found between each year.
2. Age and sex distribution
Men filed 31 of the 55 cases (56.4%), accounting for more than half of the lawsuits, and women filed 24 of the 55 cases (43.6%). The mean age of the plaintiffs was 43.8 years, ranging from three months to 78 years of age. Those aged 50 to 59 years accounted for the largest percentage of all age groups by filing 16 cases (29.1%) followed by those aged 40 to 49 in 10 cases (18.2%), children aged below 10 years in eight cases (14.5%), those aged 70 to 79 in seven cases (12.7%), and those aged 30 to 39 in six cases (10.9%).
3. Medical departments
Cases against the Department of Orthopedics had the greatest number of all malpractice claims with eight cases (10.9%) followed by the Departments of Pediatrics and Dentistry with five cases (9.1%) each, the Department of Obstetrics and Gynecology with four cases (7.3%), and the Departments of Ophthalmology, Neurosurgery, Cardiology, and Hematology-Oncology with three cases (5.5%) each. Compared to the reported number of cases at other medical institutions, PNUH had a relatively higher frequency of medical lawsuits against the Departments of Surgery, Pediatrics, and Obstetrics and Gynecology. After combining the six divisions of the Department of Internal Medicine including Cardiology, Hematology-Oncology, Infectious Diseases, Gastroenterology, Nephrology, and Pulmonology, Internal Medicine had the greatest number of cases with 13 cases in total (23.6%). However, during the study period, medical lawsuits were not filed against nine departments: Psychiatry, Dermatology, Rehabilitation Medicine, Family Medicine, Endocrinology and Metabolism, Rheumatology, Radiation Oncology, Nuclear Medicine, and Pathology.
4. Lawsuit motives
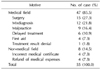
Problems related to surgical procedures accounted for the largest percentage of all motives with 15 cases (27.3%) followed by misdiagnosis with 12 cases (21.8%), inappropriate treatment with nine cases (16.4%), delayed treatment with six cases (10.9%), and emergency care with four cases (7.3%). One case filed an appeal against their prescribed treatment (1.8%). In addition, eight litigations (14.5%) occurred in non-treatment areas including inaccurate medical certificates and refunds for medical expenses. Of all of the 55 cases, the primary cause of the 21 death cases (38.2%) was surgery followed by misdiagnoses in five cases (23.8%), emergency care in four cases (7.3%), delayed treatment and malpractice in two cases (3.6%) each, and objection to medical expenses in one case (1.8%) (Table 1).
5. Time to proceedings and hearing durations
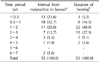
The average period required to bring the lawsuit to proceedings from malpractice was 16.5 months, ranging from one month to 6 years and 4 months. The most common time period was between 6 months and a year, during which 18 cases (32.7%) were observed. Thirteen cases (23.6%) had a period of less than six months followed by 11 cases (20.0%) with a one to two year period, seven cases (12.7%) with a two to three year period, three cases (5.5%) with a three to four year period, two cases (3.6%) with a six to seven year period, and one case (1.8%) with a four to five year period. The mean duration from the hearing to the disposition of the lawsuit was 21.7 months, ranging from one month to four years and 11 months. The duration was between one to two years in 22 cases (40.0%) followed by two to three years in 15 cases (27.3%), six months to one year in eight cases (14.5%), three to four years in five cases (9.1%), less than six months in three cases (5.5%), and four to five years in two cases (3.6%) (Table 2).
6. Final court decision
The final court decision was made by the first trial court in 31 cases (56.4%), the second trial court in 16 cases (29.1%), and the highest court in eight cases (14.5%). Final decisions were advisory conciliation in 11 cases (20.0%), compulsory mediation in 11 cases (20.0%), agreement through mediation in two cases (3.6%), and a court ruling of mediation in one case (1.8%). Mediation before trial was the most common disposition in 25 cases (45.5%). Rulings partially and completely in favor of the plaintiff were given in eight cases (14.5%) and one case (1.8%), respectively. The plaintiff won in nine cases (16.4%), and lost in six cases (10.9%). In addition, rejection and withdrawal occurred in 10 cases (18.2%) and five cases (9.1%), respectively. Overall, the most to least common final decision was mediation, court ruling, rejection, and withdrawal.
7. Amount of compensation
The total amount of compensation claimed was 8.366 billion Korean won, ranging from about 2.53 million to 966 million won. The average compensation amount per claim was about 152 million won, and the annual average compensation amount was about 146 million won. The highest amount of compensation claimed was 100 million and one thousand to 300 million won in 23 cases (41.8%) followed by 50 million and one thousand to 100 million won in nine cases (16.4%), 30 million and one thousand to 50 million won in six cases (10.9%), 10 million and one thousand to 30 million won in five cases (9.1%), 300 million and one thousand to 500 million won in four cases (7.3%), 5 million and one thousand to 10 million won in three cases (5.5%), 500 million and one thousand to 1,000 million won in three cases (5.5%), and less than 5 million won in two cases (3.6%). The highest average amount of compensation claimed was 279 million won for a malpractice suit followed by 169 million won for objection to the hospital care outcome, 160 million won for surgical errors, 147 million won for delayed treatment, and 145 million won for a misdiagnosis. The average compensation amount was lower than that for the 21 death cases, where the average amount claimed was 144 million won. The total amount of compensation paid in the death cases was about 2.27 billion won, ranging from 1.763 million to 7 million won. The actual compensation paid in these cases accounted for 22.9% of all compensation claims. The average amount decided per claim was 42 million won, and the annual average compensation amount decided was 29 million won. The highest average amount of compensation decided was zero won in 19 cases (34.5%), 10 million and one thousand to 30 million won in 12 cases (21.8%) followed by 50 million and one thousand to 100 million won in six cases (10.9%), less than 50 million won in six cases (10.9%), between 50 to 100 million won in four cases (7.3%), 100 million and one thousand to 300 million won in four cases (7.3%), 30 million and one thousand to 50 million won in three cases (5.5%), and more than 500 million and one thousand to 1,000 million won in one case (1.8%) (Table 3). According to the motives for claims, the highest average amount of compensation decided was 109 million won for malpractice followed by 48 million won for misdiagnosis, 39 million won for surgery, and 40 million won for objection to the hospital care outcome. The average compensation amount in these cases was higher than that of the 21 death cases, where the average amount decided was 24 million won. By medical department, the highest compensation amount was 210 million won in the Department of General Surgery followed by 202 million won in Pediatrics, 129 million won in Gastroenterology, and 100 million won in Urology. The ratio of compensation claimed to compensation decided was highest in General Surgery at 98.1% followed by Radiology at 84.9%, Urology at 64.2%, Thoracic Surgery at 50.5%, Nephrology at 43.6%, Pediatrics at 43.2%, Gastroenterology at 30.5%, Neurology at 24.4%, Neurosurgery 21.6%, and Anesthesiology at 20.0%.
DISCUSSION
Hospitals pursue the goal of efficiency and productivity within the complex team of administrative staff, medical practitioners, and experts who come from a wide range of fields and managed hospital protocol across various areas including investment and profit, human resources management, construction of medical centers and facilities, medical service improvement and customer satisfaction, ethical management, and public healthcare policy. Legal risks are associated with all work tasks in the hospital setting, and a wide range of efforts has been exerted in the overall operation of hospitals to minimize these legal risks. Legal risks that occur in hospitals are mainly divided into three categories: medical malpractice, patient safety management, and the illegal conduct of hospital workers. Medical malpractice comprises the implementation of preventive measures and the response to accidents. Patient safety management involves stealing, falls, personal information protection, death with dignity, and sexual assaults. Illegal conduct of hospital workers includes the creation of false medical certificates, rebate, poor medication management, the incomplete execution of work tasks, and other types of illegal conduct. Medical disputes with patients mainly occur in association with medical malpractice and safety management under legal, social, institutional, and cultural environment changes domestically. Malpractice-related medical disputes, in particular, have drawn the most attention from hospital managers and all hospital workers because of the wide range of co-existing risk factors that exist during hospital care [3]. Therefore, effective countermeasures are thought to be crucial to minimize medical disputes between medical malpractice victims and medical practitioners in hospitals with substantially different medical facilities, workforce, medical areas, and systems.
In recent years, the number of medical lawsuits has shown an increasing trend in countries including the United States, Japan, Taiwan, and others [456]. According to the 2007 Judicial Year Book in Korea, the highest number of lawsuits was recorded in 2007 with 1,104 cases, and more than 800 medical lawsuits occurred annually for the last three years since 2007.
In these domestic situations, a total of 55 civil medical lawsuits (annual mean, 4.2 cases) were filed against the PNUH and completed over the past 13 years (2000~ 2012). Although a decreasing trend in the number of filed suits was observed since 2010, a lower frequency was observed in the PNUH compare to the annual average number of lawsuits (5.6 cases) filed against national university hospitals from 2009 to 2011 in Korea. A total of 150 medical disputes were submitted to the PNUH Medical Dispute Mediation Committee and 68 of these claims did not progress to medical lawsuits through alternative dispute resolution (ADR) in the same period. The reduced frequency is anticipated to be primarily attributable to the role of the PNUH Medical Dispute Mediation Committee. Of the 55 civil lawsuits examined in the present study, only three of these claims had been deliberated and mediated by the Medical Dispute Mediation Committee; the other 52 claims had progressed to lawsuits. Therefore, systematic response measures should be established to minimize the progression of claims to lawsuits and a specialized workforce should be nurtured by evaluating the role and effectiveness of ADR. During the study period, only two criminal lawsuits related with medical malpractice occurred, showing a relatively lower frequency below 4% compared to that of civil lawsuits. In the case of claims that cannot be mediated by ADR, a public medical dispute mediation system should come into effect before claims can progress to medical lawsuits. Public ADR systems including Physicians Professional Liability Insurance (1973), the Council of Arbitration of the Korean Medical Association (KMA) (1981), the Medical Judgment Arbitration Committee of the Ministry of Health and Welfare (1982), the Korea Consumer Agency (1998), and the recently established Korea Medical Dispute Mediation Committee (2012) have been forecasted to be able to mediate medical disputes reasonably and effectively. In addition to these ADR systems, the disclosure program that was first introduced in 2001 by the University of Kentucky Hospital has been implemented in major hospitals in Korea to efficiently manage medical disputes. In the case of medical malpractice disputes, the disclosure program initiates swift investigation with transparent explanations, allowance of investigations by a third party, early recognition and apology in the case of obvious mistakes, pre-proposal for the appropriate amount of compensation, and other services. Arguably, the most successively operated disclosure program is the early disclosure and offer program at the University of Michigan Health System where medical lawsuits were reduced from 262 to 83 cases, saving litigation costs up to one million dollars from three million dollars and cutting the disposition period of dispute in half [7]. Therefore, medical dispute management methods appropriate for the actual conditions of each hospital in Korea require further attention in the future.
The extended period from medical malpractice to proceeding for malpractice suits, the duration of the hearing after the malpractice incident, and the disposition of a lawsuit imposes psychological, administrative, and financial burdens to the corresponding medical practitioners or associated departments. Furthermore, patients and their family members can be negatively affected by these proceedings. The average duration from medical malpractice to litigation was 16.5 months in PNUH, and the mean duration of the hearing after the initiation of litigation was 21.7 months. Approximately three years passed from the medical malpractice incident to the disposition of the litigation. The mean duration of the hearing was shorter than that of the medical lawsuits in Japan from 1996 (37 months) to 2008 (27 months), but was about 2.5 times longer than that of general lawsuits that occurred in 2005 in Japan (8.4 months). The duration of the medical hearings was found to be relatively longer in Japan due to the length of the required medical assessments, the existence of emotional conflicts, and for other reasons. Therefore, a range of efforts needs to be exerted to reduce the duration medical lawsuit hearings. The hearing duration was reported to be reduced by about half to 14.8 months after the initiation of the Division of Medical Malpractice Lawsuits in the Osaka District Court of Japan over five years from April 2001 to March 2006 [8]. Thus, legal systems need to apply efforts to reduce the duration of these hearings through court consultations.
According to the data on the frequency of domestic medical lawsuits by medical department reported by the Council of Arbitration of the KMA, the number of medical disputes against Obstetrics and Gynecology was the highest at 41.8% of all of the 2,870 claims followed by General Surgery at 14.8% and Orthopedics at 11.3% between 1982 and 1999 [9]. Moreover, a gradually increasing trend in the frequency of medical lawsuits was found in the Department of Internal Medicine [5,10]. According to the statistics in Japan, the Departments of Internal Medicine had the largest percentage of medical disputes at 29.6% followed by General Surgery at 21.5%, Plastic Surgery at 17.2%, and Obstetrics and Gynecology at 13.1%. These four departments accounted for about 80% of all of the disputes filed against all of the medical departments in Japan [5]. In contrast, the order of departments in PNUH with the most to least medical disputes were Orthopedics, Pediatrics, Oral and Maxillofacial Surgery, and Obstetrics and Gynecology, and the disputes filed against these departments accounted for about half of those filed against all departments. The disputes against the divisions in the Department of Internal Medicine accounted for about 25% of all disputes, which is comparable to the results from Japan. The highest frequency of medical lawsuits was generated against internal medicine. In terms of the amount of compensation awarded, the Department of Pediatrics was characterized by having a relatively higher litigation frequency and amount of compensation, which were substantially different from that in other departments or hospitals. For example, a case of hypoxic brain damage in a premature baby concluded with the highest compensation amount ever awarded in Korea. Even though compensation liability of the admitting hospital primarily falls under the scope of any side effects and other adverse events associated with medical treatments or surgical procedures, medical litigations were performed in nine cases (16.4%) due to five cases (55.6%) due to postoperative infections, 3 cases (33.3%) due to side effects after surgery, and one case (11.1%) due to delayed treatment at a tertiary medical institution. If a patient is transferred from the initially admitted medical institution or department to a different institution/department, precise treatment information about the patient's conditions should be carefully and completely communicated to patients and/or their family members, when applicable. For example, one lawsuit drew much attention from medical and legal perspectives in a patient that was initially diagnosed with breast cancer in a preoperative biopsy, but found to have no tumor tissues after an extensive mastectomy.
According to the 2001 report by the Council of Arbitration of the KMA, domestic medical lawsuits occurred most frequently after surgery (29.0%) followed by spontaneous vaginal delivery (18.1%), injection (13.6%), and therapeutic procedures (13.2%) among the 1,629 medical disputes that occurred from 1995 to 1999 [9]. In the present study, the most common cause for filing a medical lawsuit was also surgery (27.3%) followed by receiving a wrong diagnosis (21.8%), malpractice (16.4%), and delayed treatment (10.9%). However, in the actual litigation cases, the highest percentage of cause for filing a medical lawsuit was death in 38.2% of cases. Of these cases, surgery had preceded most cases (28.6%). However, the amount of compensation claimed or decided during medical lawsuits due to death was approximately 2 to 3 times higher than that of medical lawsuits due to malpractice or misdiagnosis. This finding indicates that the amount of compensation for accidental medical disputes could be higher in regular patients than severely ill patients; therefore, further attention needs to be paid in these types of disputes. According to the recently reported outcomes of the Korea Consumer Agency that mediated 328 claims associated with surgery from 2011 to August 2013, the most common type of surgery was aesthetic plastic surgery at 21.6% followed by tumor surgery at 17.1%, fracture surgery at 12.2%, spine surgery at 11.6%, and intestinal surgery at 6.7%. The most common cause for surgical accident was wrong surgery at 38.7% followed by a lack of explanation at 12.5%, and postoperative management problems at 11.6%, which accounted for more than 80% of all malpractice claims made against physicians. These findings imply that the frequency of medical lawsuits will likely increase and those physicians will be held responsible for medical liability claims in many future cases. To reduce the incidence of medical lawsuits, in-depth, pre-prevention education on accurate diagnosis and surgical procedures as well as thorough pre- and post-operative clinical practice are crucial measures for medical practitioners in departments with a particularly high frequency of medical claims. Moreover, guidelines for response measures to medical malpractice are essential. Eight lawsuits (14.5%) had been filed in non-treatment areas including medical certificates or incorrect charges for medical expenses, suggesting that healthcare administration services need to be enhanced along with medical care services.
Regarding the final disposition of the present lawsuits, the courts recommended patients to end in a settlement instead of progressing to trials, since they considered these medical malpractice claims as damages to medical consumers. For this reason, settlement accounted for the largest percentage of all dispositions at 45.5% followed by a court decision at 27.3%, in which ruling was given mostly against the plaintiffs, and rejection and withdrawal at 38%. These tendencies were observed similarly in the 9,771 medical lawsuits that occurred in Japan between 2003 and 2012. Conciliation accounted for the largest percentage at 50.5% of all cases and court decisions were made in 37.4% of all cases [5]. In the future, malpractice claims are projected to end in settlement or mediation between patients and hospitals instead of progressing to court trials in the medical disputes where conciliation court, disclosure programs, and an ADR are actively taken into consideration. This is because the negative effects of medical lawsuits have been carefully taken into consideration, such as financial loss or mental and physical exhaustion in patients and the desolation of a physician's reputation. Ultimately, these resolution schemes for medical disputes serve as a virtuous circle by reducing the overall social costs. Therefore, thorough aims grounded on scientific evidence in a case of a medical dispute are anticipated to conclude medical dispute resolution and legal decisions favorably. An upward trend was found in the annual amount of compensation claimed and decided. The total amount of compensation claimed annually surpassed 1 billion won in 2004 and 2 billion won in 2009 in malpractice claims that occurred in PNUH. The average amount claimed per claim was approximately 150 million won. The total amount of compensation decided annually exceeded 400 million won in 2004 and 1 billion won in 2009. The average amount decided per claim was approximately 40 million won. The compensation amount decided against the amount claimed was 22.9%. The ratio of compensation amount claimed to compensation amount decided was lower in Korea than that of Japan in 2008 with a court decision occurring in 37.6% and conciliation in 50% of these cases [5]. The ratio of compensation amount claimed to compensation amount decided is projected to gradually increase in Korea [11].
CONCLUSIONS
The overall service quality in hospitals in Korea should be improved and losses resulting from medical disputes in hospitals and due to medical staff could be minimized by proactively handling legal risk at the hospital management level including the medical care system. Moreover, inefficient practices and risk factors in administration service should be eliminated. The results of the present study are expected to be used as a comprehensive reference to predict and prevent medical malpractice by devising response measures to medical disputes, an accident investigation system, and response measures to litigations, which should be utilized as system and educational data for the prevention of future legal disputes in the healthcare environment. In conclusion, we propose the establishment of a more efficient and productive medical care support system with minimized hospital legal risk through the activation of the ADR by the operation of Medical Dispute Mediation Committee, the development of a legal service support center, enhancement of legal services for hospital employees, deployment of specialized human resources, and the specialization of work tasks.


 XML Download
XML Download