

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer is the second leading cause of cancer death in men in the United States [1]. Prostatectomy and radiation therapy are the preferred treatment modalities in men with localized prostate cancer. Androgen deprivation therapy (ADT) is used as an adjuvant therapy after radical prostatectomy and for the treatment of metastatic prostate cancer. Although prostate cancer is generally sensitive to initial ADT, tumors that have overcome the absence of gonadal androgens eventually regrow [2]. When prostate cancer progresses despite castration levels of testosterone, it is termed castration-resistant prostate cancer (CRPC) a term that reflects the knowledge that such cases of re-emergent prostate cancer are not independent of androgens, as was once believed. Unfortunately, recurrent tumors are more aggressive, evasive, and deadly [3], and most prostate cancer deaths are from CRPC.
Cholesterol has been implicated in the pathogenesis of diseases such as cardiovascular disease and in many forms of cancer, including prostate cancer [4]. Prostate cancer is associated with elevated levels of cholesterol, which may support cell proliferation by contributing cholesterol for membrane composition and signal transduction [5,6]. Based on these findings, several studies have explored the relationship between serum cholesterol levels and the incidence of prostate cancer and associated mortality. However, these studies have reported inconsistent results [7,8,9,10,11]. Similarly, the effects of statins on the overall risk reduction of prostate cancer remains controversial [12,13,14], with some studies suggesting that statins have no effect, while others have found statins to be associated with significant risk reduction, especially in advanced-stage tumors [15,16]. However, previous research has not addressed the relationship between levels of cholesterol and tumor progression to CRPC in patients with prostate cancer.
In this study, we aimed to investigate the potential association between hypercholesterolemia and the risk of progression to CRPC in men who have undergone ADT.
MATERIALS AND METHODS
1. Patient characteristics
After Institutional Review Board approval in Ulsan University Hospital (No. 2015-06-009), data from 314 patients who were diagnosed with prostate cancer from 2005 to 2012 were reviewed retrospectively. After excluding 160 patients who underwent radical prostatectomy or were transferred to other clinics, 154 patients who were initially treated with ADT were included. ADT was employed as a treatment modality for these patients either due to multiple bone metastases at the time of diagnosis (n=50, 32.5%) or due to old age accompanied by other morbidities (n=104, 67.5%), instead of radical prostatectomy or radiotherapy. ADT involved bilateral orchiectomy in nine patients and maximal androgen blockade including luteinizing hormone-releasing hormone agonist injection and oral antiandrogens in 145 patients. The primary outcome was the time to prostate-specific antigen (PSA) progression. In patients with castration serum levels of testosterone (<50 ng/dL), the time to PSA progression indicative of CRPC while undergoing ADT was defined as the time from the initiation of ADT to a 50% increase in PSA from its lowest level or the time from the initiation of ADT to a 25% increase in PSA levels from baseline, and was confirmed using PSA consensus criteria [17]. The mean follow-up was 34.8 months (median, 25.4 months).
2. Cholesterol levels and statin use
Patients' levels of serum cholesterol at diagnosis and statin use were reviewed. The levels of serum cholesterol were available in all patients. Cholesterol levels were categorized as hypercholesterolemia (>240 mg/dL, n=8), borderline (200~240 mg/dL, n=40) and desirable (<200 mg/dL, n=106). High- and low-density lipoprotein (HDL and LDL) cholesterol levels were not present for all patients and, therefore, were not included in the analysis. Patients who took statins before being diagnosed with prostate cancer were categorized as statin users. The statins used in these patients included atorvastatin (n=6), simvastatin (n=4), pravastatin (n=2), and rosuvastatin (n=2). The doses of statin were translated into dose equivalents based on previous published study [18], with 20 mg of simvastatin assigned a value of 1. Dose equivalents of <1, 1, and >1 were present in two patients (14.3%), nine patients (64.3%), and three patients (21.4%), respectively. The duration of statin use was not evaluated.
3. Statistical analyses
Clinicopathological characteristics were compared between patients with and without bone metastasis at the time of diagnosis using the chi-square test and the Student's t-test. Multivariate analysis was performed to evaluate the factors associated with the development of CRPC after ADT treatment. Since statin use and cholesterol could affect each other, multivariate analysis was performed again, including statin use instead of cholesterol. A subanalysis was performed according to the presence of bone metastasis at the initial diagnosis. PSA levels were measured every three months after ADT treatment. Radiographic evaluation using abdominopelvic computed tomography or pelvic magnetic resonance and radionuclide bone scanning was performed every six months and when clinically indicated. None of the patients experienced severe complications requiring the discontinuation of ADT therapy. SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses, with p-values <0.05 considered to indicate statistical significance.
RESULTS
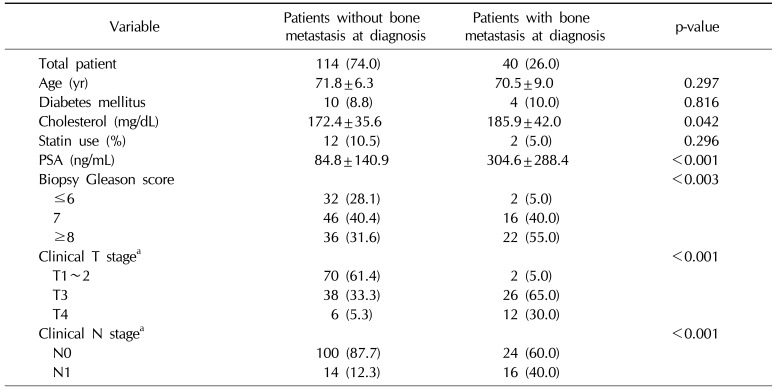
The mean age of the patients was 71.3 years old, and their mean PSA level was 141.8±212.6 ng/mL at the time of diagnosis (range, 1.5~876 ng/mL). The clinical T stage was T1 or T2 in 72 patients (46.8%), T3 in 64 patients (41.6%), and T4 in 18 patients (11.7%). The Gleason score (GS) was ≤6 in 34 patients (22.1%), 7 in 62 patients (40.3%), and ≥8 in 58 patients (37.7%). The mean level of serum cholesterol was 175.9±37.7 mg/dL and 14 patients (9.1%) were statin users. Patients without bone metastasis had lower PSA levels (84.8 ng/mL vs. 304.6 ng/mL) and lower cholesterol levels (172.4 mg/dL vs. 185.9 mg/dL) than those with bone metastasis (Table 1). Furthermore, patients without bone metastasis had lower GSs and less advanced T stage findings than patients with bone metastasis.
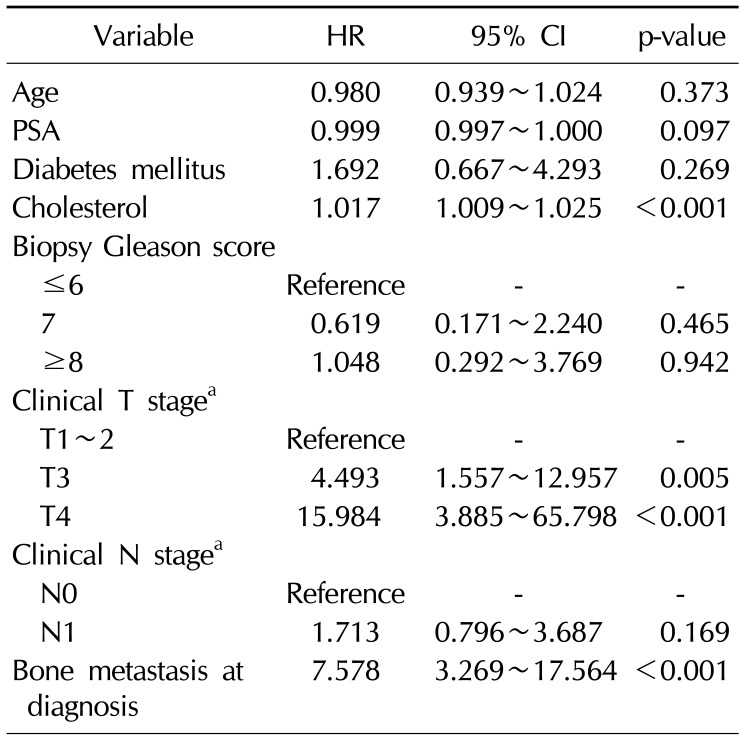
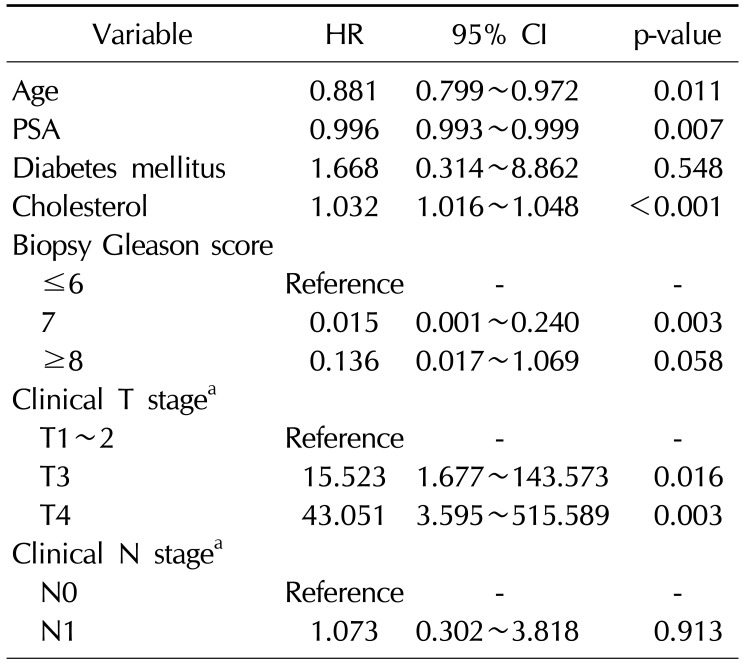
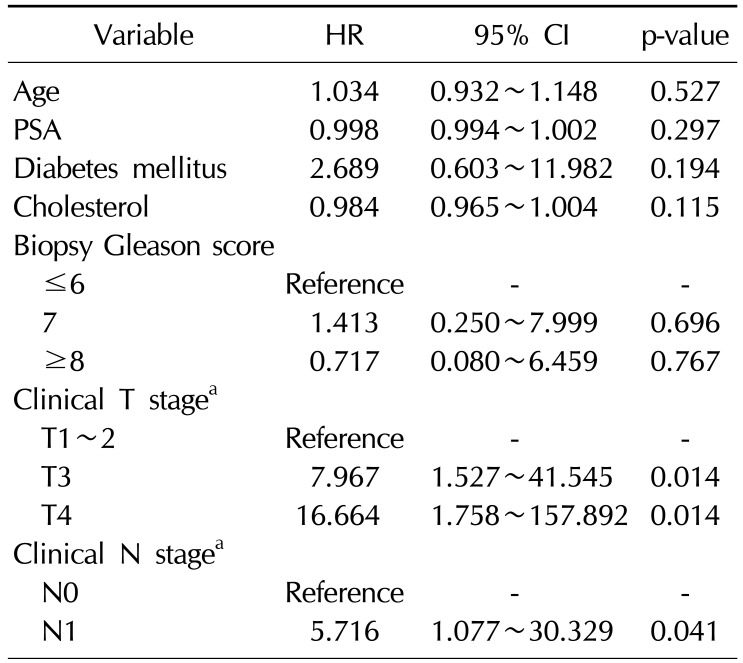
CRPC developed in 44 patients (28.6%) and the mean duration from ADT treatment to CRPC was 24.1 months. CRPC developed in 16 patients (10.4%) of the patients without bone metastasis, with a mean duration of 24.8 months, and 10 patients exhibited newly developed bone metastasis when CRPC was diagnosed. In contrast, CRPC developed in 28 patients (56.0%) with bone metastasis, with a mean duration of 23.6 months, and all patients in this group exhibited aggravated metastatic bone lesions when CRPC was diagnosed. In multivariate analysis, hypercholesterolemia was associated with the development of CRPC (hazard ratio [HR]=1.017, p<0.001), depending on the clinical T stage (HR=4.493, p=0.005 for T3 vs. HR=15.98, p<0.001 for T4), and the presence of bone metastasis (HR=7.578, p<0.001) (Table 2). Statin use was not associated with the development of CRPC. In the subanalysis, hypercholesterolemia was associated with the development of CRPC in patients with bone metastasis at diagnosis (HR=1.032, p<0.001) (Table 3). However, in patients without bone metastasis, hypercholesterolemia was not associated with the development of CRPC (Table 4).
DISCUSSION
In this cohort, patients without bone metastasis were found to have lower cholesterol levels than patients with bone metastasis. Our findings are comparable with those from other studies, which have shown an inverse association between statin use and the risk of advanced-stage and high-grade disease, with or without M1 lesions [15,16,19,20]. After excluding statin users, the inverse associations for high-grade tumors persisted. This finding suggests that cholesterol itself may play a role in pathogenesis. The mechanisms through which statins inhibit cancer processes can be classified into cholesterol-mediated and noncholesterol-mediated mechanisms [12]. Statins decrease cholesterol levels by inhibiting HMG-CoA reductase. Cholesterol is a major component of lipid rafts, which are involved in signaling pathways regulating prostate cancer cell survival and proliferation [12,21]. Additionally, statins may influence the rate of prostate cancer progression by inhibiting the synthesis of isoprenoids. In observational studies, statin use has been found to be associated with a reduced risk of aggressive prostate cancer [15,16]. However, previous studies analyzing the relationship between cholesterol levels and the incidence of aggressive prostate cancer have reported inconsistent conclusions [7,8,9,10,11]. A possible explanation for these discrepancies is the possibility that cholesterol levels in the environment of the tumor may not be reflective of serum levels.
The present study found hypercholesterolemia to be associated with the development of CRPC after ADT in patients with bone metastasis at the time of the initial diagnosis of prostate cancer. Similarly, a previous study evaluating the association of cholesterol levels with grades of prostate cancer found that men with higher cholesterol levels (>240 mg/dL) were more likely to develop highgrade or rapidly growing metastatic prostate cancer than men with desirable (<200 mg/dL) or borderline levels (200~240 mg/dL) [9]. However, in the present study, it was found that the development of CRPC was not associated with the presence of high, borderline, or desirable cholesterol levels. While cholesterol levels have been reported to increase concomitantly with the transition from non-cancerous to cancerous prostate epithelial cells [22], little is known about how this correlates with the progression to CRPC. A previous study reported that cholesterol homeostasis can be maintained during the progression of prostate cancer [23]. If CRPC cells maintain cholesterol homeostasis, cholesterol accumulation will occur during the progression to the advanced stage of prostate cancer. Thus, hypercholesterolemia at the time of prostate cancer diagnosis might imply that the disease has progressed. However, the relationship between hypercholesterolemia and tumor progression has not yet been fully elucidated. It has not been conclusively determined whether initiating cholesterol-lowering drugs (statins) after the diagnosis of prostate cancer is capable of delaying disease progression.
In this study, statin use was not associated with the development of CRPC (data not shown). Furthermore, the type and dose of statin were not associated with the development of CRPC. However, considering the cholesterol-lowering effect of statins and the fact that previous studies have demonstrated an association between statins and less progressive prostate cancer, it is possible that further studies with larger populations may lead to meaningful results.
This study has some limitations. First, the present study included a relatively small sample size and was a retrospective study. Second, LDL and HDL cholesterol levels were not analyzed. LDL cholesterol levels are more strongly associated with prostate cancer recurrence after radiotherapy than total cholesterol levels [24]. Nonetheless, our study suggested that hypercholesterolemia may be associated with the development of CRPC in patients with bone metastasis at the time of diagnosis. Clinicians may wish to consider cholesterol levels as a prognostic factor in metastatic prostate cancer before starting ADT treatment.
 XML Download
XML Download