

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Priapism is defined as a persistent and painful erection lasting longer than four hours without sexual stimulation, and usually needs emergency management [1]. Since the first reported case by Tripe in 1845 [2], the etiology and clinical condition of priapism have been clarified gradually. Some epidemiological studies have reported the incidence of priapism to be 0.3 to 1.0 per 100,000 males per year [234]. Typically, priapism occurs frequently in patients aged 40~50 years [3]. Although the causes differ based on the clinical type of priapism, most cases are idiopathic (21%, alcohol drinking or drug abuse; 12%, perineal trauma; and 11%, sickle cell disease [SCD]) [5].
Based on episode history and pathophysiology, priapism is classified into three subtypes: ischemic (low-flow), non-ischemic (high-flow), and stuttering (intermittent) priapism. Stuttering priapism is characterized by a recurrent and intermittent erection, frequently occurring in a specific patient population with SCD, and is categorized as a self-limited ischemic priapism. As ischemic and non-ischemic priapism differ based on treatment options and emergency status, it is important for urologists to discriminate between the types.
Go to : 
DIFFERENTIAL DIAGNOSIS
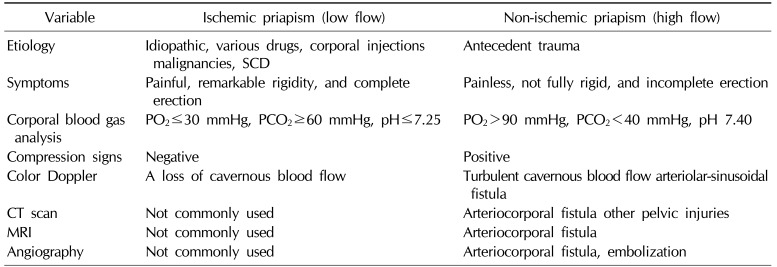
Differential diagnoses for ischemic and non-ischemic priapism are indicated in Table 1, and a flowchart of each treatment option is shown in Fig. 1.
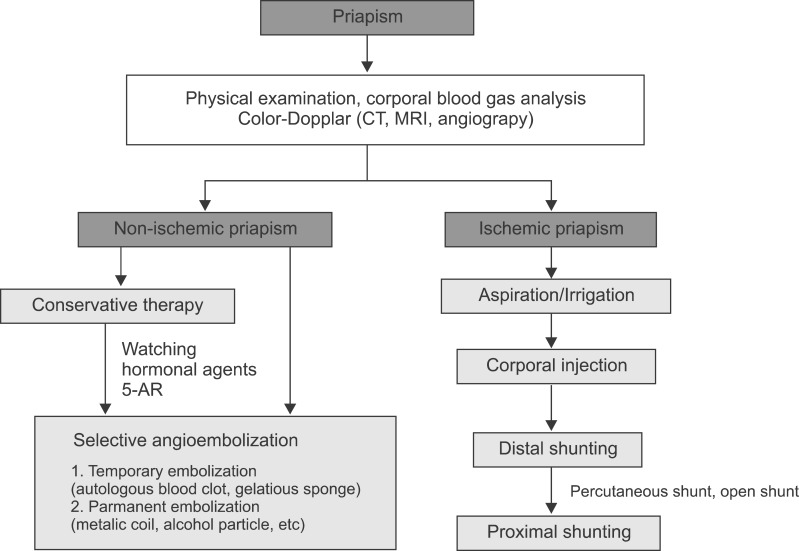 | Fig. 1Flowchart of treatment options for ischemic and non-ischemic priapism. CT: computed tomography, MRI: magnetic resonance imaging, 5-AR: 5-alpha reductase inhibitors.
|
Table 1
Differential diagnosis of priapism
![]()
1. Ischemic priapism
Ischemic priapism, which accounts for 95% of all priapism cases, is the most common type [1]. It is characterized by a persistent, painful erection with remarkable rigidity of the corpora cavernosa caused by a disorder of venous blood outflow from this tissue mass. Thus, penile tissue shows a hypoxic and acidotic condition, similar to penile compartment syndrome, within the closed space of the corpora cavernosa. Because it can lead to corporal tissue damage with time, emergency examination and management are required; delayed treatment can result in complete erectile dysfunction (ED) [1].
The most common causes of priapism are iatrogenic, such as intracarvernosal injections of prostaglandin E2 or papaverine hydrochloride and overdose administration of phosphodiesterase 5 (PDE5) inhibitors used in ED treatment [16]. Some previous reports have stated that psychiatric medications, alpha-1 blockers, leukemia, malignant lymphoma, malignancies (metastasis of the bladder, prostate, and colorectal carcinoma of the corpora cavernosa), SCD, and idiopathic causes lead to the development of ischemic priapism [25789]. Possible mechanisms of this type of priapism may be delay in corporal venous dilation, increase in blood stickiness, and direct venous invasion of malignancy.
The diagnosis of ischemic priapism can be made by a cavernous blood gas analysis to confirm the storage of venous blood within the corpora cavernosa manifesting as a lower partial oxygen pressure (pO2; <30 mmHg), higher partial carbon dioxide pressure (pCO2; >60 mmHg), and a decline of pH (<7.25) [2]. A cavernous blood gas analysis is recommended to distinguish non-ischemic from ischemic priapism. In addition, a blood analysis should be performed for determining the cause of priapism and its management, regardless of the type of priapism. Reticulocyte counts and hemoglobin electrophoresis are informative for signifying the presence of SCD [2]. Color Doppler ultrasonography (CDU) is also a useful tool for screening ischemic priapism, which shows a loss of cavernous blood flow without a cavernous arterial pulse [10]. Computed tomography (CT) is not commonly used for the diagnosis of ischemic priapism, but CT should be performed for identifying its etiology for management of the disease.
2. Non-Ischemic priapism
Non-ischemic priapism manifests as a painless, persistent, partially rigid, and nonsexual erection. It is caused by excess blood flow from arteries into the corpora cavernosa. As cavernous tissue shows a well-oxygenated condition, non-ischemic priapism is not considered a medical emergency.
Non-ischemic priapism is generally less prevalent compared to ischemic priapism; however, it is relatively frequent in regions with rare prevalence of SCD [5]. Non-ischemic priapism is usually the result of antecedent trauma of the perineal or penile regions. It is induced by arterial damage leading to arteriocorporal fistulas and occasionally to a trauma-associated pseudoaneurysm [111213] contributing to excess unregulated arterial flow to the corpora cavernosa. In general, an incomplete and partially hard erection does not develop immediately after the trauma but occurs later.
In non-ischemic priapism, the corporeal blood gas analysis reveals normal arterial blood gas values of PO2 >90 mmHg, PCO2 <40 mmHg, and pH 7.40 [2]. Perineal compression, which is also known as a compression sign and results in obstruction of the causative arteriocorporal fistulas, contributes to detumescence of the erection. Compression sign is sometimes indicative of a diagnosis of non-ischemic priapism, complementing a physical examination [14]. CDU is also a common diagnostic tool and can show the unregulated and turbulent cavernosal arterial flow within the corpora cavernosa, suggestive of the presence of arteriolar-sinusoidal fistula in most non-ischemic priapism cases [15]. Enhanced CT or CT angiography can be non-invasively and quickly performed, and these are secondary recommended examinations for non-ischemic priapism. In addition, localization of arteriocorporeal fistulas within the corpora cavernosa and the presence of other pelvic injuries can be determined [16].
Internal pudendal arteriography is not used for the initial diagnosis of priapism because of its invasiveness, but it is an essential examination for cavernosal arterial embolization. The penile arteriography reveals outflow of the contrast medium into the corpora cavernosa from the arterial– sinusoidal fistula. As there are some cases with bilateral arteriocavernous fistula, internal pudendal arteriography should be performed bilaterally.
3. Stuttering priapism
Stuttering priapism is caused by SCD and is a recurrent and intermittent painful erection. SCD is most prevalent in sub-Saharan Africa, tribal regions of India, and the Middle East, whereas it is less prevalent in East Asia, including Japan and Korea [18]. The lifetime incidence rate of priapism in the SCD population is as high as 42%, and these episodes result in ED in over 30% of cases [19]. In over 75% of cases of stuttering priapism, patients with SCD experience their first episode of priapism in their 20s, and conversely, the most common cause of priapism occurring in children is SCD [19]. On the other hand, stuttering priapism may also be idiopathic or drug-induced and may finally lead to ischemic priapism, and the diagnosis and clinical management are generally based on ischemic priapism.
A cause of stuttering priapism in men with SCD is suggested by the relatively low PDE5 levels caused by less activity of endothelial nitric oxide (NO), leading to the release of neuronal NO, which can contribute to abnormal relaxation of the corpora cavernosa [20].
Go to :
CLINICAL MANAGEMENT
The goal of clinical management for priapism is to make the continuous erection fade away and to preserve the ability to have erections in the future. Therefore, emergency evaluations to determine whether the priapism is ischemic or non-ischemic are required to initiate the appropriate management. The differentiation can initially be made based on the patient's history and physical examination. Subsequently, confirmation must be obtained with cavernous blood gas analysis and radiologic assessment. The objective in clinical management of ischemic priapism, which is an emergency that may result in permanent ED, is to remove the compartment condition of the ongoing cavernosal hypoxia. Conversely, non-ischemic priapism is not a surgical emergency because of the absence of cavernosal hypoxia. The goal of intervention is solely to cure the persistent erection and to recover normal erectile ability in response to sexual desire and activity.
1. Ischemic priapism
Once the diagnosis of ischemic priapism has been made, emergency management is required. Less invasive intervention should be initiated.
1) Corporal aspiration
After penile anesthesia, a 19-gauge needle is used to puncture the corpus cavernosum at the lateral shaft of the penis to avoid damaging the urethra and the dorsal neurovascular bundle [521]. In cases of ischemic priapism, corporal aspiration reveals dark venous blood initially and should be continued until bright red oxygenated blood is aspirated [5]. When aspiration is difficult because of the increased viscosity of the blood within the corpus cavernosum, cold saline irrigation can promote evacuation of the viscous hypoxic blood [22]. Aspiration alone, with or without corporal irrigation, has a success rate of approximately 30% [223].
2) Corporal injection of sympathomimetics
If the corporal aspiration procedure is not successful, sympathomimetics should be instilled into the corpus cavernosa. Because of their low risk profile for any cardiovascular side effects, α-adrenergic agonists such as phenylephrine, with minimal β-adrenergic effects, should be used [22324]. Continuous monitoring of vital signs during administration of these agents is important, especially in patients with cardiovascular diseases [2425]. Phenylephrine, which has been reported as the most commonly used sympathomimetic, is diluted in normal saline to a concentration of 200~500 µg/mL and given in 1-mL doses every 5~10 minutes up to a maximal dose of 1 mg until recovery from the continuous penile erection [2025]. Alternatively, ephedrine hydrochloride (5~10 mg), epinephrine (20~80 µg), or norepinephrine (20~80 µg) diluted in 5 mL of normal saline can also be used [23]. These sympathomimetics are less effective in patients with ischemic priapism continuing over 6 hours because of the severe acidosis within the corpora cavernosa [20]. Aspiration with the use of sympathomimetics, with or without corporal irrigation, can result in an increase in the efficacy rate for ischemic priapism of 43% to 81% [219].
3) Surgical management
Ischemic priapism continuing for more than 48 hours is difficult to resolve by corporal aspiration, irrigation, and sympathomimetic injection. Thus, more immediate surgical shunting should be considered as another management option in such cases (Fig. 2). The goal of surgical shunting is to make an iatrogenic fistula to drain the pooled deoxygenated blood from the corpora cavernosa.
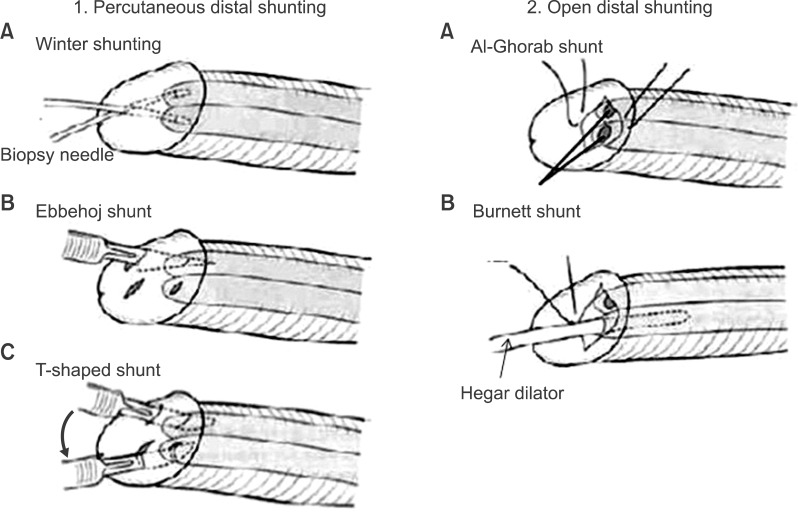
(1) Percutaneous distal shunting
A percutaneous distal shunt, which is the procedure for creating a fistula between the glans penis and corpora cavernosa, should be attempted first, because it is easier to perform and has the fewest complications. Distal shunting is usually achieved by inserting a biopsy needle from the glans to the corpora cavernosa (Winter's shunt) [26], or a scalpel (Ebbehoj shunt) [27]. Another type of shunting (T-shaped shunt) procedure involves inserting a scalpel into the corpora cavernosa from the glans, followed by a 90° lateral rotation of the scalpel and then pulling it out [28]. Pooled dark venous blood and coagula should be removed out of the corpora cavernosa until bright red blood is revealed from the penile shunting wound.
(2) Open distal shunting
The traditional surgical approach (Al-Ghorab shunting) is a dorsal subcoronal incision, which is performed by excising a piece of the tunica albuginea at the tip of the corpus cavernosum [22930]. Burnett developed a technique involving dilatation of the cavernous tissue using a Hegar dilator (Burnett shunting) [31]. Some previous reports have noted that open distal shunting causes no more erectile failure than that caused by ischemic priapism itself, and shows excellent success rates even in patients who failed treatment with percutaneous distal shunting [2932].
(3) Proximal shunting
If distal shunts are unsuccessful, proximal shunts, such as corporospongiosal shunts (Quackels shunt) [33] and corpora-saphenous shunts (Grayhack shunt) [34] can be considered, although these procedures are associated with some complications including ED, local thrombus formation, and pulmonary embolism. The success rate of proximal shunts is 50% to 70% [2].
4) Penile prosthesis
Some previous reports mention the efficacy of a penile prosthesis for patients with ischemic priapism not responding to conventional management [3536]. As long-term failure to treat low-flow priapism contributes to cavernosal fibrosis with resultant penile induration and shortening, immediate insertion of a penile prosthesis is recommended for maintaining penile length [35]. Rees et al [35] suggest immediate penile prosthesis insertion in acute ischemic priapism as a treatment option with minimal complications.
2. Stuttering priapism
Stuttering priapism is a recurrent form of ischemic priapism in which unwanted, painful erections occur repeatedly with intervening periods of detumescence. Therefore, its medical management is generally equivalent to that of ischemic priapism. For preventing recurrence of stuttering priapism, hormonal therapy using gonadotropin-releasing hormone agonists, estrogens, anti-androgens, and 5α-reductase inhibitors has been a successful medical management option [37].
Men with SCD have a defective PDE5 regulatory function in the penis, resulting in abnormal relaxation of the corpora cavernosa due to the release of neuronal NO [20]. PDE5 inhibitors can contribute to improving unregulated signaling of the NO pathway in patients with SCD, and long-term efficacy of oral PDE5 inhibitors in men with SCD-associated priapism without affecting normal erectile capacity has been shown [3738]. The efficacy of PDE5 inhibitors is usually seen within 2~4 weeks.
3. Non-ischemic priapism
As cavernous tissue shows a well-oxygenated condition in non-ischemic priapism, it is not considered a medical emergency. Therefore, observation is recommended as the initial management [2]. Some conservative treatments such as ice and site-specific compression to the injury are included as part of the observation therapy. Indeed, Hakim et al. described that ischemic priapism could be resolved with no further management, and erectile function of these patients could be retained sufficiently for sexual intercourse with no negative sequelae [41]. A previous report suggested that observation can be recommended for 6 weeks, and clinical symptoms and CDU should be checked every 2 weeks [42]. However, insufficient information regarding conservative therapy has been available. There has been no evidence to support the recommended duration of observation. Further discussion regarding conservative treatment is likely to be required.
Aspiration with or without injection of vasoconstrictive agents is not recommended and should be used solely for the diagnosis of non-ischemic priapism [2]. Sympathomimetic agents are not therapeutically effective but may result in significant adverse effects to the cardiovascular system. A temporary therapeutic response to intracavernous methylene blue, which is known to antagonize endothelial-derived relaxation factors, has been reported [243].
Although 60% to 70% of cases with non-ischemic priapism show spontaneous resolution, ED may occur in approximately 30% of patients among those with long-term clinical observation [22144]. Therefore, for cases that fail to respond to conservative treatments, selective angioembolization of the arterial–sinusoidal fistula should be considered. Since Wear et al [45] reported a case with non-ischemic priapism treated successfully by occlusion of the left internal pudendal artery with an autologous clot, several embolization materials, both temporary (autologous blood clot, absorbable gel, and gelatinous sponge) and permanent (metallic coil, n-butyl-2 cyanoacrylate, and polyvinyl alcohol particles), are currently available [219444546]. Generally, temporary materials are commonly used for first-line embolization because of the relatively lower subsequent incidence of ED [444546]. Overall, angioembolization shows a high efficacy rate of 90% [244748], whereas there are reports of an unsatisfactory curative rate of 60% to 70% by initial embolization. A decrease in erectile function caused by embolism occurs in 32.0% of cases within 1 month after treatment, in 40.0% within 1~3 months, in 16.0% within 3~6 months, and in 12.0% after more than 6 months; finally, permanent ED occurs in <10% of non-ischemic priapism cases.
An autologous blood clot is the safest and ideal embolism material because it causes only a temporary interruption of the blood flow feeding the fistula owing to its premature lysis. Gel foam can also interrupt the arterial blood flow temporarily, similar to a blood clot, and the effects usually last 5~6 weeks after injection [46]. Therefore, temporary materials are initially preferred in most cases. However, cases with arterial embolism using absorbable materials often have recurrence of priapism, with the recurrence rate reported to be 30% to 40% [4445464748].
Permanent materials can contribute to a more durable occlusion than absorbable materials, which can achieve a lower recurrence of priapism. However, there is a risk of post-interventional permanent ED, especially in cases of bilateral fistula. The permanent materials should be alternatively used for selected cases that fail to respond to treatment using primary temporary materials. A recent, improved technique of angiography has been shown to contribute to decreased development of ED by permanent embolism, which has been reported to be equivalent to that of temporary embolism [4748].
Furthermore, hormonal agents such as anti-androgens, 5α-reductase inhibitors, and gonadotropin-releasing hormone agonists have been suggested as additional options for conservative treatment of some patients. Nocturnal penile tumescence (NPT) may disturb the cure of priapism, and these agents can be used to prevent NPT [19]. However, minimal information regarding the efficacy and safety of these agents is currently available. Because these therapies can have negative effects on erectile function and fertility, especially in young patients, long-term use of hormonal agents is not recommended.
Go to :
CONCLUSIONS
The goal of the management of priapism is to achieve detumescence of persistent penile erection and to preserve erectile function after resolution of the priapism. Therefore, despite the low incidence of priapism, prompt evaluation and emergency management often are required. Many previous clinical studies have contributed to cultivating a better understanding of the pathophysiology, diagnosis, and management of priapism. Urological clinicians should address this emergency condition to achieve successful treatment.
Go to :
 XML Download
XML Download