

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Penile necrosis may accompany health problems such as disseminated infections and circulatory disorders. Ischemia of the penis is relatively rare because of its excellent collateral vessels [1]. Until recently, a surgical procedure such as penectomy was the only treatment option. The cure rate of conservative management was low. We report a case of diabetes mellitus (DM)-associated penile necrosis with severe multiple atherosclerosis, for which treatment by balloon angioplasty and a bypass graft was successful. Additional intracavernous injections (ICI) of prostaglandin E1 (PGE1) facilitated the circulation of blood flow, which was very important to stimulate penile healing.
CASE REPORT
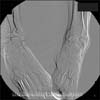
The patient was a 64-year-old man with type II DM and hypertension who complained of severe pain with ongoing penile necrosis (Fig. 1). The patient had received local wound care for the ischemic penile lesions at another urologic clinic for 2 months. The urethral meatus and ventral portion of the penis were dusky and covered by necrosis with discharge. He also had severe intermittent pain in both legs because of unknown cause. Thus, we performed pelvic and penile arteriography.
Severe calcification and tortuosity were visible in the common and external iliac arteries. Both internal iliac arteries were diffusely narrowed and the blood flowed sluggishly. The pudendal arteries were occluded proximally, leaving the penile vessels invisible (Fig. 2), and the arterial flow was almost invisible in both legs (Fig. 3). We concluded that atherosclerosis was the cause of the penile necrosis and claudication of the legs. We planned to perform an operation jointly with a vascular surgeon. Percutaneous transluminal angioplasty of the left common iliac artery was carried out for dilatation of the vessel by Seldinger method. Under fluoroscopic guidance, a balloon catheter was introduced into the narrow portion and then inflated using water pressure. Both femoral vessels were exposed through a vertical groin incision. Atheromatous plaques were found in the common, superficial, and deep femoral arteries. Endarterectomy was performed for treatment of leg claudication. We excised the necrotic site and sutured it with the tension-free method. A simple meatotomy was performed at the stenosis of the urethral meatus.
Postoperatively, we decided to try PGE1 via ICI to improve penile blood flow. An injection of 5 µg PGE1 was infused into the penile cavernous bodies once daily for 4 weeks. At 3 weeks after beginning the PGE1 treatment, the necrotic eschar of the penile glans peeled off and glans of penis had transformed into a yellowish color, and at 4 weeks the necrotic penile color was pinkish (Fig. 4). At end of the 4 weeks, PGE1 treatment was stopped. There were no significant complications. Two years of follow-up computed tomography angiography showed a partial occlusion of both iliac arteries and the femorofemoral graft site. The patient remained pain-free without recurrence of penile necrosis on follow-up seven years postoperatively, but DM-associated cerebral and myocardial infarction occurred.
DISCUSSION
Penile ischemia and necrosis can be caused by a penile prosthesis, severe DM, thrombotic phenomena, and calcium deposits in patients on dialysis. Necrosis of the penis is rare because of its abundant blood circulation [1]. Atherosclerosis is a common complication in type II DM patients. The buttocks, thighs, and lower abdominal region are more common ischemic sites by atherosclerosis than the penis because of their small blood vessels [2]. Our patient had severe penile necrosis and no arterial pulsations in either foot.
DM-associated penile ischemia commonly progresses to gangrene [3]. Our patient had type II DM, which can contribute to blood vessel narrowing, thereby disrupting the blood supply to the penis and both legs. If early surgical treatment such as penectomy for penile necrosis is done, the gangrenous progression of the penis may be preventable [3]. In addition, we believe that early vascular intervention with appropriate patient selection was effective in restoring blood flow to the penis. Intra-arterial contrast angiography is considered to be the gold standard for the evaluation of patients with arterial occlusive disease [4]. It may be of help in penile revascularization. Balloon angioplasty and femoral bypass was potentially helpful to walk, if claudication with multiple atherosclerosis which has failed to respond to conservative treatment should be treated by an intervention such as percutaneous balloon angioplasty and femorofemoral bypass [4]. We operated on the stenotic lesions of the iliac arteries with balloon angioplasty to restore blood flow to the penis, and on the femoral arteries by femorofemoral anastomosis to restore blood flow to both legs. In this patient, not only the penile necrosis, but also the claudication of both legs were alleviated after the operation. ICI therapy using PGE1 is an effective treatment for erectile dysfunction in patients with organic or psychogenic erectile dysfunction [5]. It was used to frequently in the management of erectile dysfunction because of its vasoactive mechanism. It has shown a high cure rate in patients with erectile dysfunction [5]. In this case, ICI PGE1 in the form of 5 µg Caverject (Pharmacia & Upjohn Inc., Bridgewater, NJ, USA) was used daily for 4 weeks to facilitate the flow of blood and stimulate the healing of the penis. At 3 weeks after beginning the PGE1 treatment, the necrotic eschar of the glans penis peeled off and the glans transformed into a yellowish color, and at 4 weeks the formerly necrotic portion of the penile was pinkish. There were no other complications.
Vascular assessment may improve the evaluation and treatment of penile ischemia with multiple vessel occlusion. Intervention of multiple atherosclerosis was effective in relieving the vessel clogging and restoring blood flow to the penis. In addition, PGE1 therapy was very helpful in improving the remaining penile ischemic lesions. These procedures may reduce the need for penectomy in treating penile ischemia.



 XML Download
XML Download