

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aging Asian men commonly experience lower urinary tract symptoms suggestive of benign prostatic hyperplasia (BPH-LUTS) [1,2,3], which can substantially affect their quality of life (QoL) [2]. These symptoms include daytime urinary frequency, urgency, and nocturia (classified as storage/irritative symptoms) and straining, weak stream, intermittency, and incomplete emptying (classified as voiding/obstructive symptoms) [4]. While BPH-LUTS is common in both Korean and non-Korean men, the reported prevalence varies [5] because of heterogeneity in study outcomes, study design, study populations, and definitions of terms (e.g., LUTS versus BPH-LUTS) [6]. Although a few studies have reported ethnic differences, most studies have reported similar prevalence rates of BPH-LUTS in Asian and Caucasian men [3,6,7]. BPH-LUTS often coexists with erectile dysfunction (ED), and the prevalence and severity of both conditions increase with age, with the severity of one condition often being associated with that of the other. Furthermore, when men seek treatment for one condition, they are often found to have both [6].
Until recently, treatment options for BPH-LUTS in Korea mainly included α-blockers and 5-α-reductase inhibitors either as monotherapy or in combination [5,8]. The selective phosphodiesterase type 5 inhibitor tadalafil was approved in Korea as an on-demand and once-daily treatment for ED in 2003 and 2008, respectively. Tadalafil has also been shown to be an efficacious and well-tolerated treatment for BPH-LUTS in Asian [9,10,11] and largely Caucasian [12,13,14,15] study populations, and it was approved in Korea for once-daily treatment of BPH-LUTS in 2012.
One small, placebo-controlled study in Korean men with BPH-LUTS [16] and two larger placebo-controlled Asian studies with Korean subpopulations [10,11] have supported tadalafil as an efficacious and well-tolerated treatment. However, tadalafil has not been assessed previously in a large sample comprising only Korean men. Therefore, an integrated analysis of Korean participant data from three studies of tadalafil [10,11,16] was conducted to assess the efficacy and safety of tadalafil in a large Korean population with BPH-LUTS.
MATERIALS AND METHODS
1. Description of included studies
1) Study design
This is a post hoc integrated analysis of data from Korean study participants receiving placebo or tadalafil 5 mg once daily in three 12-week, randomized, double-blind, placebo-controlled studies of tadalafil in Asian men with BPH-LUTS [10,11,16]. For each study, the protocol was approved by the Institutional Review Board at each site, and each study was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent.
2) Study population
The eligibility criteria for the individual studies were largely similar and have been described previously [10,11,16]. Men aged ≥45 years with a total International Prostate Symptom Score (IPSS) ≥13 and bladder outlet obstruction of intermediate severity (urinary peak flow rate [Qmax] ≥4 and ≤15 mL/s) were enrolled in the studies. The main exclusion criteria were prostate-specific antigen >10.0 ng/mL (or ≥4.0 ng/mL if prostate cancer could not be ruled out) and bladder postvoid residual volume (PVR) ≥300 mL.
4) Outcomes
The primary objective was to compare the change in total IPSS from baseline to week 12 [17] after treatment with tadalafil versus placebo. The secondary objectives were to compare the following between the tadalafil and placebo groups: change in total IPSS from baseline to weeks 4 and 8; change in IPSS voiding subscore, IPSS storage subscore, and IPSS QoL index from baseline to weeks 4, 8, and 12; and Patient Global Impression of Improvement (PGI-I) and Clinician Global Impression of Improvement (CGI-I) at study endpoint (week 12 or early discontinuation visit). Safety assessments included the incidence of treatment-emergent adverse events (TEAEs) and the changes in PVR from baseline to endpoint. In addition, the change in Qmax from the baseline to the endpoint was assessed; Qmax was an efficacy parameter in two studies (Studies 1 and 2) and a safety parameter in one study (Study 3).
2. Integrated analysis
Data from Korean study participants receiving placebo or tadalafil 5 mg once daily in the three studies were included in this integrated analysis. Treatment differences in total IPSS, IPSS voiding subscore, IPSS storage subscore, and IPSS QoL Index at weeks 4, 8, and 12 were assessed via mixed-effects model repeated measures (MMRM) analysis (primary analysis), with the treatment group, study, visit, centered-baseline, visit-by-treatment interaction, and centered-baseline-by-treatment interaction as covariates. The mean least squares (LS) changes from the baseline for each treatment group and for the treatment difference, and two-sided 95% confidence intervals for the treatment difference were calculated for each of these IPSS parameters. In addition, the treatment differences in the IPSS parameters from the baseline to the endpoint were assessed by an analysis of covariance (ANCOVA; secondary analysis) based on the last observation carried forward, with the terms for centered-baseline, study, treatment group, and centered-baseline-by-treatment interaction as covariates. The treatment differences in PGI-I and CGI-I were assessed by performing the Cochran-Mantel-Haenszel test adjusted for baseline LUTS severity. The treatment differences in Qmax were assessed using ANCOVA. The treatment differences in PVR were assessed using ANCOVA (for comparing mean values) and the Wilcoxon rank-sum test (median values). A two-sided significance level of 0.05 was used for all analyses, and all analyses were performed using SAS Drug Development version 3.4 (SAS Institute, Cary, NC, USA).
RESULTS
1. Participant disposition
Of the 1,373 randomized participants in three Asian studies of BPH-LUTS, 354 Korean participants received placebo (177 participants) or tadalafil 5 mg once daily (177 participants) in the integrated analysis (Fig. 1). In Study 1 [16], 51 Korean participants received placebo and 51 received tadalafil 5 mg; in Study 2 [10], 44 Korean participants received placebo and 47 received tadalafil 5 mg; and in Study 3 [11], 82 participants received placebo and 79 received tadalafil 5 mg. Of the 354 Korean participants, 330 participants (93.2%) completed the studies.
2. Demographic and baseline clinical characteristics
The demographic and baseline clinical characteristics of the integrated analysis population were largely similar in the placebo and tadalafil groups (Table 1). The mean age (±standard deviation [SD]) of the participants was 62.5±7.08 years, and 39.3% of the participants (139/354) were ≥65 years. The mean (±SD) total IPSS was 18.0±5.99, and 38.4% of the participants (136/354) had severe LUTS (IPSS ≥20).
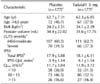
3. Total International Prostate Symptom Score
A significantly greater improvement (p<0.001) in the total IPSS for the change from baseline to week 12 was observed for tadalafil versus placebo (LS mean: tadalafil=-5.97; placebo=-3.94), according to the results of a primary MMRM analysis (Table 2, Fig. 2). This result was confirmed by the results of a secondary ANCOVA analysis, which showed a significantly greater improvement (p=0.001) in the total IPSS for the change from the baseline to the endpoint for tadalafil versus placebo groups (data not shown). In addition, significantly greater improvements in the total IPSS for the change from the baseline to weeks 4 (p<0.001) and 8 (p=0.002) were observed for tadalafil versus placebo groups, as assessed by an MMRM analysis (Table 2, Fig. 2).
4. International Prostate Symptom Score voiding subscore, International Prostate Symptom Score storage subscore, and International Prostate Symptom Score quality of life index
Significantly greater improvements (p<0.05) in the IPSS subscores from the baseline to weeks 4, 8, and 12, and in the IPSS QoL Index from the baseline to weeks 8 and 12, were observed for tadalafil versus placebo groups, as indicated by the results of the primary MMRM analysis (Table 2). These results were in good agreement with those of the secondary ANCOVA analysis, which showed significantly greater improvements (p<0.05) in the IPSS subscores and the IPSS QoL Index from the baseline to the endpoint for tadalafil versus placebo groups (data not shown).
5. Patient Global Impression of Improvement and Clinician Global Impression of Improvement
Improvements in urinary symptoms were observed, as rated by both the patients and the clinicians. There was a significant difference among treatment groups in the distribution of participants over the PGI-I response categories (p<0.001) and a numeric difference among treatment groups in the distribution of participants over the CGI-I response categories (p=0.127). The proportion of participants who felt that their urinary symptoms were improved was 68.4% (117/171) in the placebo group and 84.7% (144/170) in the tadalafil group. The proportion of clinicians who felt that their patients' urinary symptoms were improved was 72.5% (124/171) in the placebo group and 79.4% (135/170) in the tadalafil group.
6. Peak urine flow rate and postvoid residual volume
The mean change in Qmax from the baseline to the endpoint was not significantly different (p=0.945) between the placebo (LS mean: 2.30 mL/s) and the tadalafil (LS mean: 2.30 mL/s) groups. The mean change in PVR from the baseline to the endpoint was significantly different (p=0.009) between the placebo (LS mean: 1.6 mL/s) and the tadalafil (LS mean: -7.2 mL/s) groups, favoring tadalafil. However, an additional non-parametric analysis of the median change in PVR was conducted because of concerns that the data were not normally distributed; this analysis did not show a statistically significant difference (p=0.269) between the placebo (median: 1.0 mL) and the tadalafil (median: 0 mL) groups.
7. Safety and tolerability measures
A higher proportion of the participants experienced ≥1 TEAE in the tadalafil group (12.4%) than in the placebo group (7.9%) (Table 3). Four participants in the tadalafil group discontinued because of an adverse event (AE): myalgia (2 participants; both considered treatment-related), back pain, and pleural effusion. Two participants in the tadalafil group experienced three serious adverse events (SAEs). One participant experienced metastatic lung adenocarcinoma and pleural effusion, and the other participant experienced lumbar spinal stenosis; none of these SAEs was considered by the investigator to be treatment-related. There were no reports of AEs associated with sexual dysfunction.
DISCUSSION
In this large sample of Korean men with BPH-LUTS, the use of tadalafil 5 mg once daily for 12 weeks improved LUTS compared with the use of the placebo, as demonstrated by the significant improvements in the total IPSS, IPSS subscores, and the IPSS QoL index. The observed improvement was significant at the first visit after 4 weeks of treatment (apart from the IPSS QoL index, which was numerically improved). Significant improvements in urinary symptoms were observed at the study endpoint for tadalafil versus placebo, as assessed by the PGI-I, with numerical improvements observed for the CGI-I. There were few AEs, and no new safety concerns were identified. The findings of this integrated analysis support tadalafil as an efficacious and well-tolerated therapy in Korean men with BPH-LUTS.
The improvement in total IPSS observed for tadalafil compared with placebo in this Korean population was clinically meaningful and is largely consistent with that observed in other 12-week studies of tadalafil 5 mg in Asian [9,10,11] and Caucasian [13,14,15] study populations. The magnitude of placebo-adjusted improvement in the total IPSS from the baseline to week 12 in this Korean population (mean LS: tadalafil=-5.97; placebo=-3.94) is slightly larger than that observed in a recent study involving only Japanese males (tadalafil=-4.9; placebo=-3.8) [9]. However, compared with subjects in the Korean population, those in the Japanese study were generally older and had less severe symptoms; furthermore, a larger proportion of the Japanese patients was previously treated with an α-blocker. These factors may have contributed to the observed difference in the total IPSS improvement between the two studies. Hence, combined with the findings of the Asian and Caucasian study populations [9,10,11,13,14,15], the results of this integrated analysis provide further evidence for the efficacy of tadalafil in the treatment of BPH-LUTS in different ethnic populations.
The significant improvements in total IPSS, IPSS voiding subscore, and IPSS storage subscore for the tadalafil versus placebo users in this Korean population were apparent after 4 weeks of treatment, and they continued to be evident throughout the 12-week treatment period. The magnitude of improvement at 4 weeks was largely similar to the changes observed after 12 weeks, suggesting that tadalafil is effective in the early stages of treatment. Numerical [11,14] and significant [15] improvements in (modified) IPSS for tadalafil versus placebo users have been observed after 1 and 2 weeks of treatment in individual studies.
A comparison of the placebo-controlled results of this integrated analysis of tadalafil with the published results of the effect of α-blockers in Korean men with BPH-LUTS is difficult due to the differences in the study population, study design, treatment duration, and lack of placebo-run period or a placebo control [5]. In two randomized, placebo-controlled tadalafil studies including Korean men with BPH-LUTS, the improvement in total IPSS observed with the α-blocker tamsulosin (0.2 mg) compared with that of tadalafil (2.5 or 5.0 mg) was numerically smaller in one study (Study 1) [16] and numerically larger in the other study (Study 2) [10]. However, these studies were not powered to identify the difference between the active therapies.
In line with the improvements in total IPSS and IPSS subscores in this Korean population, the IPSS QoL Index also improved during the treatment period, with a numerical improvement after 4 weeks and a significant improvement after 8 and 12 weeks. This suggests that although most patients may experience almost all of the observed maximum treatment effect after 4 weeks (as assessed by total IPSS and IPSS subscores), a significant impact on QoL may be observed after 8 weeks of treatment.
The impression of improvement in urinary symptoms at the endpoint was apparent in a majority of the subjects treated with either tadalafil or placebo, as assessed by the participant (PGI-I) or the clinician (CGI-I). A significantly larger proportion of the subjects had the impression of an improvement when treated with tadalafil than with the placebo, whereas a numerically larger proportion of clinicians had the impression of improvement when treating with tadalafil than with the placebo. This suggests that PGI-I is possibly a better instrument to identify placebo-adjusted changes than CGI-I, which has not undergone the same validation as PGI-I [18].
Tadalafil treatment did not significantly improve the mean Qmax compared with placebo in this integrated analysis population, which is consistent with most individual studies of tadalafil 5 mg in Asian [9,10,11] and Caucasian [12,13,14,19] study populations and with studies of α-blockers in Asian study populations [10,16,20]. In a recent integrated analysis of Qmax changes in more than 1,100 predominantly Caucasian men with BPH-LUTS, the median improvement using tadalafil compared with that using placebo was statistically significant, but the changes were numerically small and not considered clinically meaningful [21]. The severity of bladder outlet obstruction at the baseline in the integrated analysis of Caucasian men was more severe (Qmax<10 mL/s: placebo, 48.1%; tadalafil, 45.5%) [21] than the baseline assessment in the current integrated analysis of Korean men (Qmax<10 mL/s: placebo, 36.9%; tadalafil, 31.5%), which should be considered when evaluating the different outcomes of the two integrated analyses. However, according to the American Urology Association BPH treatment guidelines, there is poor correlation between changes in Qmax and improvement in symptoms [22], and small numerical changes in Qmax are believed to have a limited impact on any improvement in BPH-LUTS [21]. Other factors such as smooth muscle relaxation in the bladder neck, prostate, and urethra; increased blood perfusion and oxygenation of bladder and prostate tissue; and decrease in afferent nerve activity are believed to be of greater importance in this regard [14,23].
The safety findings in this Korean population are consistent with those reported in previous studies of tadalafil in Asian [9,10,11,16] and Caucasian [12,13,14,15] populations with BPH-LUTS, as well as with the prescribing information for tadalafil [24]. Tadalafil was well tolerated in this Korean population, with few participants discontinuing because of an AE. In addition, the proportion of participants receiving tadalafil and reporting TEAEs was relatively low, and there were few SAEs, none of which was considered to be treatment-related. More importantly, none of the TEAEs were associated with sexual dysfunction, which is in contrast to the other drug therapies for BPH, such as α-blockers and 5-α-reductase inhibitors [5]. Tadalafil is the only drug currently available in Korea for the treatment of both BPH-LUTS and ED that is not associated with sexual side effects.
The integrated analysis of three similarly designed studies allowed a large population of Korean men to be evaluated and provided a more robust analysis than that available from each individual study. While it may have been preferable to conduct one large, well-powered study of the Korean population, the results of this integrated analysis are consistent with those of other 12-week studies of tadalafil 5 mg in Asian and Caucasian study populations [9,10,11,13,14,15]. Because the treatment duration of all three studies was 12 weeks, no conclusions on the long-term efficacy and safety of tadalafil in Korean men with BPH-LUTS could be drawn from this integrated analysis. However, open-label extension studies conducted in Japanese [9] and largely Caucasian [25] populations have shown sustained efficacy and no unexpected safety findings over a 12-month period.




 XML Download
XML Download