

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
With the increase in the average human life span, the morbidity of chronic diseases such as hypertension and diabetes has also increased [1]. In addition, testosterone levels in men decrease with age as a result of declining adrenal and testicular function [2]. Consequently, studying the impact of this decrease in testosterone on chronic diseases has become important. Testosterone decreases in men induce decreases in muscle mass and increases in the amount of fat, particularly visceral fat [3]. As a result, abnormalities in glucose and lipid metabolism develop along with increased insulin resistance [4,5]. This series of events is generally referred to as the metabolic syndrome and is known to increase the incidence rate of cardiovascular diseases.
Cardiovascular diseases are among the most common causes of death in older adults [6,7]. Past studies comparing males and females in similar age ranges have shown that high testosterone levels are related to the occurrence of cardiovascular diseases [8,9,10]. Despite a few negative results, recent large-scale cohort analyses suggest that low testosterone levels are associated with coronary artery disease [11,12]. Type-2 diabetes and obesity are also associated with low testosterone levels and contribute to increased cardiovascular disease risk. Lifestyle habits such as drinking and smoking, additional factors that increase incidence rates of cardiovascular disease, also induce low testosterone levels in men [13,14,15].
The Framingham risk score (FRS), a scoring system derived using data from the Framingham heart study conducted in the United States (US), is an instrument that uses simple past medical history and gender-specific cholesterol levels in asymptomatic patients to predict the incidence rate of cardiovascular diseases in the next 10 years [16,17]. In the present study, we used the FRS to study the effect of testosterone levels on cardiovascular disease risk in patients with sexual dysfunction.
MATERIALS AND METHODS
This retrospective study included patients who visited the urology clinic between 2003 and 2013. A total of 308 patients with completed surveys, high fidelity medical records, and planned laboratory tests were selected and analyzed. This study was approved by the Institutional Review Board of Hallym University Kangdong Sacred Heart Hospital.
History taking and a physical examination including the 15-item International Index of Erectile Function (IIEF) were performed on all patients. Mean blood pressure was recorded after three measurements with the patient in a stabilized state. Laboratory tests included complete blood cell count, liver function tests, hemoglobin A1c, total testosterone, sexual hormone binding globulin (SHBG), and serum prolactin. Because testosterone fluctuates throughout the day, samples were collected before 10:00 a.m. irrespective of the season. Vermeulen's formula (available at http://www.issam.ch/freetesto.htm) was used to calculate free testosterone and bioavailable testosterone levels.
The FRS is calculated on the basis of age, gender, total cholesterol, smoking status, high density lipoprotein (HDL) cholesterol, and systolic blood pressure (SBP). The FRS was calculated using an online calculator provided by the National Heart, Lung, and Blood Institute (available at http://cvdrisk.nhlbi.nih.gov/calculator.asp). An individual with an FRS of 12 is considered to have a 10% risk of coronary heart disease in the next 10 years. An FRS of 15 indicates a 20% rate, and an FRS of 17 indicates an incidence rate of greater than 30%.
Statistical analysis was performed using IBM SPSS Statistics version 19 (IBM Co., Armonk, NY, USA). Spearman's correlation analysis was carried out for clinicopathological data relevant to testosterone. A multiple linear regression analysis was used to identify hormones and clinicopathological parameters that affected the FRS. All statistical results showed a 95% confidence interval and were considered significant when the p value was below 0.05.
RESULTS
The mean age of the 308 enrolled patients was 49.42±10.73 years, and the mean body mass index (kg/m2) was 25.07±3.14. The patients' mean total IIEF score was 28.44±18.06; the mean scores on the individual domains of the IIEF are presented in Table 1. The median total testosterone level was 3.2 ng/mL (interquartile range [IQR]: 2.3~3.2 ng/mL), and the median SHBG level was 39.06 nmol/L (IQR: 26.93~56.00 nmol/L). The median calculated free testosterone level was 0.052 ng/mL (IQR: 0.039~0.070 ng/mL), and the median calculated bioavailable testosterone level was 1.30 ng/mL (IQR: 1.00~1.76 ng/mL).
The study included 88 current smokers (38.6%) and 52 (22.8%) ex-smokers. The patients' mean SBP based on three measurements at a stable state was 126.00±16.76 mmHg. The median total cholesterol level was 184.96 mg/dL (IQR: 151.75~207.25 mg/dL), and the median HDL cholesterol level was 47.05 mg/dL (IQR: 38.75~53.25 mg/dL). The mean FRS for the study population on the basis of these values was 10.47±6.45 (Table 1).
The FRS showed a tendency toward a negative correlation with total testosterone and calculated free testosterone. However, these negative correlations were not statistically significant in Spearman's correlation analysis (p=0.064 for total testosterone, Fig. 1A; p=0.074 for free testosterone, Fig. 1B). A correlation between the total testosterone level and the total IIEF score was also not statistically significant (p=0.311), nor was the correlation between the FRS and the IIEF (p=0.143).
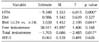
In the multiple linear regression analysis that included total testosterone and free testosterone, a significant negative correlation was observed between the total testosterone level and the FRS (p=0.017, Table 2). However, the free testosterone level was not significantly correlated with the FRS in the multiple linear regression analysis.
DISCUSSION
We found a negative correlation between the total testosterone levels in men and the risk of cardiovascular disease. Testosterone is a steroid hormone from the androgen group [18]. Although a small amount is produced in tissues other than the testicles, most testosterone is produced in the male testicles [19]. Many studies to date have reported a negative correlation between testosterone levels and the metabolic syndrome, whereby patients with low testosterone levels show elevated levels of serum triglycerides, total cholesterol, lower density lipoprotein cholesterol, apolipoprotein B, and fasting and 2-hour plasma insulin concentrations, along with decreased levels of HDL cholesterol [20]. Such changes in the lipid profile have been known to increase the risk of cardiovascular disease [21].
The IIEF is a globally used questionnaire for determining both the diagnosis and the treatment effect of sexual dysfunction. However, because the IIEF was developed to assess the impact of phosphodiesterase-5 inhibitors on erectile dysfunction, its results may not be relevant to the actual measurement of serum testosterone levels [22,23]. No significant relationship between the serum total testosterone level and the IIEF was observed in this study. This result contradicts the results of a recently published study showing a weak association between the IIEF and the total testosterone level [24]. This discrepancy may be the result of the differences in inclusion criteria. The above study targeted patients with a measured total testosterone concentration of less than 3.5 ng/mL, whereas we enrolled patients irrespective of their testosterone concentration.
The FRS is a gender-specific scoring system used to predict an individual's cardiovascular disease risk in the next 10 years [16,17]. The FRS was revised in 2008 to include cerebrovascular events, peripheral artery disease, and heart failure. The benefit of the FRS is the ability to calculate the 10-year cardiovascular disease risk by using simple medical history and cholesterol levels and to be able to advise patients to stop smoking and change their diets in order to lower their cardiovascular risk by reducing their cholesterol levels. However, because the FRS targeted the upper middle-class population of Massachusetts in the US, there is a tendency for risk overestimation in Asian (including Korean) and European contemporary populations [25]. The recent recalibration of the FRS as a coronary heart disease prediction model in Korea could be helpful for future studies of the relationship between testosterone and cardiovascular diseases [26].
Although a negative correlation between testosterone levels and the coronary artery score has been reported [21], few studies have evaluated decreases in cardiovascular disease risk following testosterone replacement therapy. In a recent study, no definite proof of reduced cardiovascular disease risk was shown in patients who received testosterone replacement therapies when compared with a placebo group [27]. Thus, a prospective study of the effect of testosterone replacement therapy is necessary. The thesis of a lowered cardiovascular disease risk through a changed metabolic profile (via changes in central obesity, insulin resistance, and lipid profile) and through changed testosterone concentrations suggests that scoring systems such as the FRS may be very helpful for future studies.
This study had the limitations of being a single-institute, retrospective study. Second, the study only included patients who visited the urology department for erectile dysfunction between 2003 and 2013. Because this may induce a selection bias, an additional broader study is thought necessary. However, patients with relevant medical records were selected for participation, and the amount of data lost was controlled as much as possible. Third, the FRS used in this study may overestimate the cardiovascular risk in Koreans because it was developed for a US population. Finally, we lacked longitudinal data on changes in the FRS or lipid profile after testosterone replacement therapy.
CONCLUSIONS
The present study found a negative correlation between the total testosterone level and the FRS. This result suggests that high testosterone levels are associated with a low 10-year risk of cardiovascular disease. However, these findings are based on data from 308 patients with erectile dysfunction and thus, require further exploration in prospective larger-scale studies.


 XML Download
XML Download