

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Testosterone replacement therapy (TRT) for the treatment of testosterone deficiency syndrome (TDS) has been widely used in the South Korea for decades.1 The aim of TRT is to establish a physiologically normal concentration of serum testosterone to correct for androgen deficiency, relieve its symptoms, and prevent long-term sequelae. The target organs of testosterone exist throughout the whole body and include the skin, muscle, liver, kidney, brain, bone marrow, and male reproductive organs.2 However, in terms of the prostate, TRT has possible side effects including development of prostate cancer and worsening symptoms of benign prostatic hyperplasia (BPH), because prostate growth is dependent on the presence of androgens, and androgens play an important role in the development of BPH. Nevertheless, there is no direct correlation between serum testosterone levels in men and the risk of developing prostate cancer.3,4 Furthermore, there are no compelling data suggesting that TRT contributes to worsening of lower urinary tract symptoms (LUTS) or promotion of urinary retention.5 Instead, an increasing body of literature with short-term follow up has recently demonstrated positive effects on LUTS and uroflow parameters.6-9 We therefore evaluated the correlation between TRT and LUTS for patients who had been treated with TRT for over a year, in patients with TDS concomitant with moderate LUTS. To the best of our knowledge, this is the first data published on this issue particularly in a Korean population.
Go to : 
MATERIALS AND METHODS
1. Institutional strategy for TRT
Between January 2006 and January 2011, 383 patients underwent TRT using intramuscular injection of 1,000 mg of testosterone undecanoate (Nebido™, Bayer Pharma AG, Berlin, Germany) in our institution. The institutional policy for initiation of TRT was the complaint of erectile dysfunction as the main symptom of TDS with a serum testosterone level less than 3.5 ng/ml. For all, a complete medical history regarding concomitant medical disease and medication from other departments or institutions was carefully taken and physical examination was performed. To estimate the efficacy of TRT, serum testosterone levels were routinely measured during the first visit, then 3, 6, and 12 months later; the time of blood sampling was 7 AM to 11 AM. The amount of total and free testosterone were measured separately, both by radioimmunoassay. Also, the changes in symptoms induced by TDS were assessed by a self-administered aging male symptoms (AMS) questionnaire, which was performed again routinely a year after TRT. The exclusion criteria for TRT in our institution were a prior history of treated hypogonadism, history of prostate cancer, active systemic disease, human immunodeficiency virus, psychosis, or history of sleep apnea. In case of initial prostate specific antigen (PSA) over 4.0 ng/ml, TRT was selectively performed for the pathologically confirmed BPH cases.
2. The main assessment of prostatic status
To investigate the baseline status of the prostate, patients underwent transrectal ultrasonography to determine the prostate volume, serum PSA, uroflowmetery parameters including maximal flow rate, voiding volume, and post-voiding residual urine. The International Prostate Symptom Score (IPSS) questionnaire was performed before TRT. In the IPSS questionnaire, the storage symptom score was defined as the sum of items 2, 4 and 7 and the voiding symptom score was defined as the sum of items 1, 3, 5, and 6. The serum PSA, uroflowmetry, and IPSS were routinely re-evaluated a year after TRT, except for a case of a complaint of aggravation of LUTS that required clinical assessment for the status of the prostate. According to the decision of the treating physician, BPH medications including alpha blockers or phytotherapy were additionally administered after initiation of TRT. However, 5-alpha reductase inhibitor was not used during TRT. At the beginning of this series, we did not have any regular restriction on the usage of LUTS medication during TRT, considering the potential development or aggravation of prostatic disease.
3. Patient selection and statistical analysis
Among all potential subjects, 246 patients who had completed a minimum of a year of follow up, with a normal digital rectal examination and PSA level of less than 4 ng/ml, and had undergone a prostate evaluation after a year of TRT were recruited for this study by retrospective chart review. In addition, another group of 17 patients who had moderate LUTS, which was defined as an initial IPSS over 8 points but below 19 with a maximal flow rate of at least 10 ml/s, but who did not take any BPH medication or use of phosphodiesterase type 5 inhibitors daily during testosterone replacement were selected from the 246 cases of TRT. Then the outcomes were assessed separately for the two groups.
The primary end point of this study was changes in the IPSS and uroflowmetry parameters including maximal flow rate (Qmax), voiding volume, and post voiding residual urine (PVR) during a year. Secondary efficacy and safety was assessed according to changes in serum testosterone, AMS score, Body Mass Index (BMI), and serum PSA.
For statistical analysis of the whole patient, to evaluate the goodness-of-fit, the Kolmogorov-Smirnov test was performed first, then Wilcoxon's signed rank test or a paired t-test was performed to compare several parameters before and after TRT. In the 17 selected cases with LUTS without BPH medication, the changes in each parameter were compared by Wilcoxon's signed rank test, assuming p<0.05 to be significant. To compare the no-BPH medication patients and their counterparts, the Mann-Whitney U test was applied. All statistical analyses were performed using SPSS™ version 17.0 (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
1. Outcomes from 246 patients with a year follow up
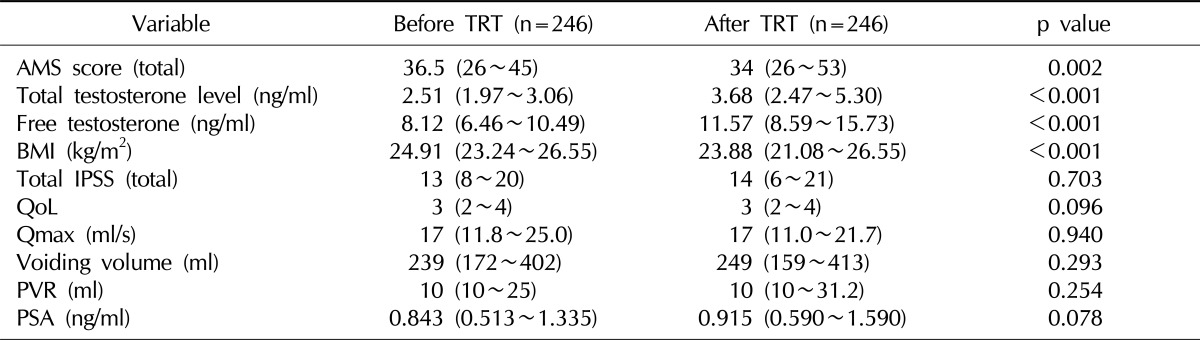
The median age with interquartile range (IQR) of the 246 patients with TRT was 58.5 (52~64.2) years old and the mean follow up period for TRT was 14.7 (13~19.3) months. Before TRT, the median (IQR) total and free testosterone levels were 2.51 (1.97~3.06) ng/ml and 8.12 (6.46~10.49) ng/ml, respectively. The median baseline prostate volume was 24.2 (19.7~29.7) ml.
After a year of TRT, the AMS score and serum testosterone level including total and free testosterone were significantly increased (Table 1). The BMI was also significantly decreased compared to baseline (p<0.001). In contrast, the IPSS and uroflowmetry parameters did not show any significant change from the baseline status. Interestingly, the serum PSA level remained unchanged after a year of TRT (p=0.078).
2. Outcomes from the 17 patients with moderate LUTS without BPH medication
The median (IQR) age of the 17 patients was 53 (52~63) years old, and median follow up period during TRT was 15.1 (14~16) months. In all of the patients, the total and free testosterone increased after TRT, and this change was statistically significant (Table 2). However, the change in AMS score and BMI was not significant in this patient group (p=0.154 and 1.000, respectively).
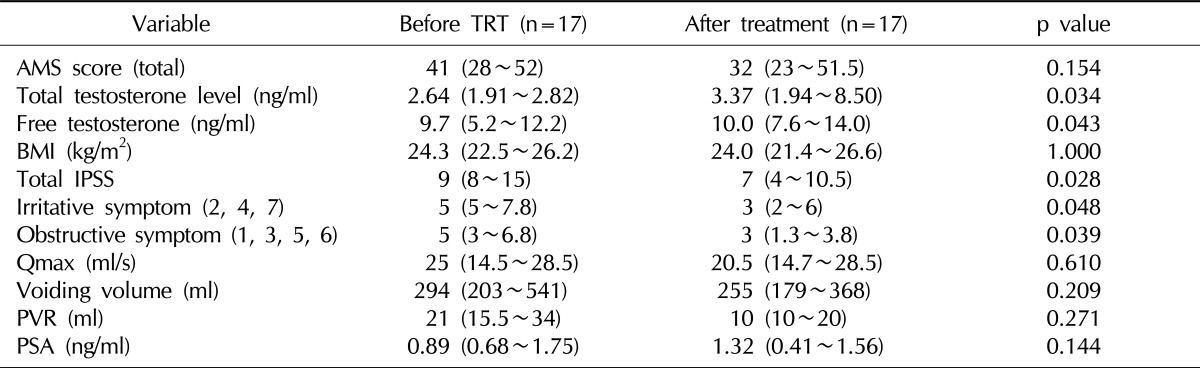
Table 2
Comparison of parameters at baseline and after TRT in 17 selected patients with moderate LUTS without BPH medication
Values are presented as mean (range).
TRT: testosterone replacement therapy, LUTS: lower urinary tract symptom, BPH: benign prostate hyperplasia, AMS: aging male symptom, BMI: body mass index, IPSS: International Prostate Symptom Score, Qmax: maximal flow rate, PVR: post voiding residual urine, PSA: prostate specific antigen.
![]()
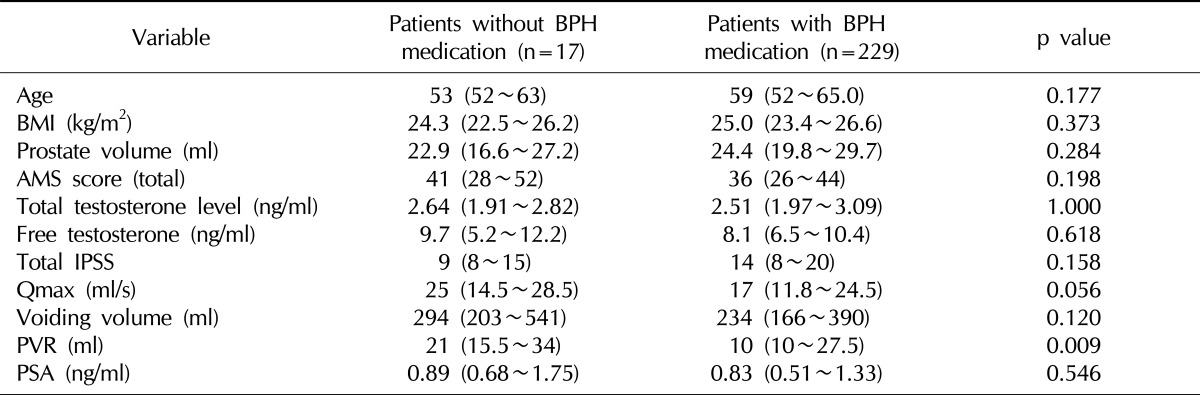
Regarding the prostate status, when comparing with the counterpart group (n=229), these selected 17 patients with moderate LUTS without BPH medication had similar baseline prostate characteristics in all variables including prostate volume, IPSS, Qmax, voiding volume, and serum PSA except PVR, but increased PVR in the no-BPH medication group (21 ml vs. 10 ml, Table 3). All of the selected patients had a minimal Qmax over 10 (10.84~45) ml/s.
The total IPSS had decreased significantly in the no-BPH medication group (p=0.028). One patient with a baseline prostate volume of 27.2 ml had reported an increased IPSS score from 10 to 12, and one patient with a baseline prostate volume of 31 ml had an unchanged IPSS score of 11. However, the maximal flow rate from both patients was maintained above 20 ml/s during TRT. Other than these two cases, the IPSS score was diminished in the rest of the patients, both in storage symptoms (items 2, 4, and 7) and voiding symptoms (items 1, 3, 5, and 6; Table 2). However, uroflowmetery variables including Qmax and PVR were maintained after a year of TRT. The serum PSA level also remained unchanged (p=0.144). No patients experienced urinary retention, BPH-related surgery, or admission for urinary tract infection during follow up.
Go to :
DISCUSSION
Although contraindications for testosterone supplementation in aging men are controversial due to the lack of large-scale studies, the greatest concerns for contemporary TRT are potential side effects on the prostate. It is well-known that the presence of androgen is required for the development of BPH, and antiandrogen agents can decrease prostate volume in patients with BPH,10 suggesting that TRT could result in worsening of LUTSs. However, recent research on the relationship between TRT and the progression of LUTS revealed outcomes opposite these traditional concerns. Tenover6 performed a short-term clinical study using 100 mg of testosterone enanthate every 3 weeks for 3 months and reported that short-term TRT did not significantly increase prostate volume or PVR. From a double-blind controlled study design, Holmäng et al7 indicated that TRT contributed to an increase of 12% in volume of the prostate gland after 8 months of treatment, but did not affect urodynamic data or IPSS. Similarly, in a double-blind placebo-controlled study, Marks et al8 demonstrated that 6 months of testosterone administration normalized serum androgen levels in aging men with hypogonadism but had little effect on prostatic tissue androgen levels or on their urinary symptoms and urodynamic data. Recently, Shigehara et al9 reported the outcome from a year-long randomized control study on 42 patients with TDS concomitant with LUTS, demonstrating improvement not only in IPSS but also in Qmax only by TRT.
In this study, we found that TRT for hypogonadal men with moderate LUTS could contribute to improvement of subjective LUTS. IPSS sub-scores also showed improvements both in storage (2, 4, 7) and voiding (1, 3, 5, 6) symptoms. On the other hand, there was no statistical difference in terms of uroflowmetery parameters including Qmax, the relatively higher Qmax in our selected group may have affected the outcomes. Like the outcomes reported by other researchers, the serum PSA level remained unchanged, and it is noteworthy that no clinical progression of BPH including urinary retention, surgery for BPH, or admission for urinary tract infection occurred during more than a year of follow up.
Possible explanations for the improvement of LUTS and bladder function by testosterone therapy have been suggested. Indeed, there are several similarities in the etiologies of erectile dysfunction and LUTS, such as metabolic syndrome, autonomic nervous activity, nitric oxide (NO) activity, and rho-kinase activity.11 Testosterone has been shown to have an effect on rho-kinase activity, and rho-kinase activity in the urinary tract may at least in part depend on testosterone.12 Increased rho-kinase activity coincides with the development of LUTS in aging men with BPH, and inhibition of rho-kinase in the rat model is thought to decrease prostatic smooth muscle cell proliferation and to decrease adrenergic contractions.13 NO is also one of the mediators of dilatation of the urethra and bladder neck.11 Chamness et al14 reported that testosterone had an effect on NO synthase in the urinary tract and suggested the possibility of improving urinary symptoms by increasing NO production.
By an uncontrolled prospective study, Karazindiyanoğlu and Cayan15 indicated that TRT significantly increased maximal bladder capacity and compliance, and decreased detrusor pressure at maximal flow, based on the results of pressure-flow analysis.15 Celayir16 observed the changes in rabbit bladder tissue after bilateral orchiectomy and demonstrated that testosterone injection significantly increased bladder capacity and compliance. By observing bladders of castrated rats receiving androgen therapy for 28 days, Madeiro et al17 had reported improvement in terms of the number of vessels, epithelial thickness, and quantity of muscular fibers compared to untreated controls. Cayan et al18 reported that, in rats, testosterone treatment resulted in a significantly higher bladder smooth muscle/collagen ratio than controls. These findings suggest that TRT can affect bladder muscle contractility and compliance.
This study had inherent limitations mainly due to its retrospective study design, including absence of urodynamic studies and follow up prostate volume after a year. Also, the small number of the patients with moderate LUTS without BPH medication lessened the power of the statistical analysis. The relatively highly maintained Qmax in the 17 selected men may bias the outcome toward a more favorable direction. In addition, the relatively high follow up loss rate of this study among 383 TRT men (29.5%) may also have biased the outcome toward positive results. Finally, due to the absence of a placebo group, we cannot draw conclusions about the subjective improvements, particularly in the Qmax without TRT, and the constitutive impact on LUTS. This is the reason that a larger prospective study design is still required on this issue, considering the lifelong impact of contemporary TRT.
Go to :
CONCLUSIONS
Over a year of TRT for selected patients with moderate LUTS and no BPH medication improved both storage and voiding symptoms, without causing clinical progression of BPH or increasing PSA. Thus, TRT can be a safe strategy even in TDS patients with moderate LUTS but maintaining a relatively high uroflow rate.
Go to :
 XML Download
XML Download