

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Paratesticular fibrous pseudotumor was first reported by Balloch in 1904. The incidence of fibrous pseudotumor has been reported to comprise approximately 6% of paratesticular lesions and tumors [1]. Mostofi and Price [2] used the term 'fibrous pseudotumor' for all of these proliferations with a peak incidence in the third decade of life, but they can occur at any age. Jones et al [3] proposed a classification for benign fibrous proliferations of the paratesticular region and testis on the basis of the benign or malignant nature of the lesions and segregated them into various categories based on location, pathologic features, and immunohistochemical studies. We describe a case of an elderly male presenting with a painless inguinoscrotal nodule.
CASE REPORT
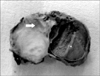
A 78-year-old male who had a medical history of hydrocele formation five years earlier presented to our institution with a hard nodule in the left inguinoscrotal region that had existed for three years. The patient had not sought any medical treatment for the hydrocele and it had resolved spontaneously. On physical examination, the nodule was mobile, hard, and non-tender and measured 3 cm in diameter. A radical orchiectomy was performed, and the nodule, along with the testis and spermatic cord, was excised out through an inguinal incision (Fig. 1). Grossly, the testis, cord, and nodule could be identified separately. The cord was thick and nodular over an area of 2.5×2.5 cm, and a cut section of the nodule was solid and grey-white. On microscopic examination, the lesion showed spindle-shaped cells with a round-to-oval nucleus and a moderate quantity of eosinophilic cytoplasm with indistinct cytoplasmic margins (Fig. 2A, 2B). Sections from the testis, epididymis, and vas deferens were unremarkable. On immunohistochemistry, the cells were reactive with smooth muscle antigen and muscle specific actin (Fig. 2C, 2D), and negative for S-100, keratin, and CD34. A final diagnosis of paratesticular fibrous pseudotumor was made.
DISCUSSION
The category of benign fibroblastic proliferations of the paratesticular region was expanded by Hollowood and Fletcher [4]. The benign fibroblastic proliferations of the paratesticular region mainly include paratesticular fibrous pseudotumours and paratesticular inflammatory pseudotumors. Paratesticular fibrous pseudotumours are adherent to the spermatic cord or epididymis, and they are characterized by multiple or solitary nodules or plaques with no age predilection. Paratesticular inflammatory pseudotumors are also described as pseudosarcomatous myofibroblastic proliferation or proliferative funiculitis. Paratesticular inflammatory pseudotumors may mimic malignancy and usually present as solitary lesions of the spermatic cord but rarely occur in a testicular or epididymal location. They are characterized by a densely arranged myofibroblastic proliferation with heterogeneous inflammatory cells and intermixed hyalinized and hypercellular areas [5].
The various synonyms used for paratesticular fibrous pseudotumors are nodular fibrous proliferation and chronic proliferative periorchitis [6]. A history of hydrocele, trauma, or infection supports a reactive pathogenesis [6]. Our case also had a past history of hydrocele formation. The cell of origin for fibrous pseudotumors appears to be the fibroblast or myofibroblast, which is supported by immunohistochemical studies performed in our case.
The differential diagnosis of fibrous pseudotumor of the testicular tunics includes fibroma of the tunics, idiopathic fibromatosis, solitary fibrous tumor, leiomyoma, and neurofibroma. The morphologic appearance of the lesion, presence or absence of an infiltrative border, and the findings of immunohistochemical studies are useful in distinguishing these entities. The true benign fibrous neoplasms arising from the paratesticular region or testicular tunics and intratesticular region are 'benign gonadal stromal tumor of the testis of spindle fibroblastic type', 'testicular stromal tumor with myofilaments', and 'fibroma of the testicular tunics' [7-9]. A differential diagnosis of fibroma of gonadal stromal origin should include unclassified sex cord-stromal tumors with prominent fibromatous components. This exclusion is important as these tumors can act in a malignant manner. Fibroma of the testicular tunics is also considered to be a true benign neoplasm; however, it lacks an association with hydrocele, trauma, or infection, as concluded by Parveen et al [9].
Paratesticular fibrous pseudotumours may present as nodular or diffuse masses, which may simulate malignancy clinically. The various paratesticular malignant tumors occurring in adults are rhabdomyosarcoma, leiomyosarcoma, liposarcoma, fibrosarcoma, malignant fi brous histiocytoma, and metastatic carcinomas. Since paratesticular fibrous pseudotumors may mimic any of these malignant tumors clinically, surgical management is the treatment of choice for these lesions. In view of a strong clinical suspicion of malignancy in our case, radical orchiectomy was performed. Although excision of the mass with preservation of the testis is the preferred surgical method, radical orchiectomy may be necessary because of difficulty in removing the lesional tissue while preserving the testis [10]. In such situations, the role of an intra-operative frozen section may be of paramount importance, and it would help if both the surgeons and pathologists are aware of fibrous pseudotumors in the paratesticular region [10]. Awareness of this entity combined with intra-operative frozen section may prevent performance of an unnecessary radical orchiectomy, especially in younger patients.

 XML Download
XML Download