

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Although a variety of tumors may arise in the scrotum since the scrotum consists of skin, smooth muscle, vessels, and nerves, scrotal tumors are infrequent. Shwannomas, which may occur in any region of the body, are very rare in the scrotum. To our knowledge, few cases have been reported, particularly extrascrotal and intrascrotal schwannoma with multiple lesions. We report a case of multiple schwannomas of the scrotum with a review of the literature.
CASE REPORT
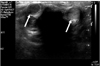
A 67-year-old man presented with a 2-year history of multiple slowly growing painless lumps in the scrotum. He did not have any history of trauma or infection. His medical history was unremarkable. Physical examination revealed (Fig. 1A) multiple non-tender, hard lumps measuring about 1×1×1.5 cm at the extrascrotal mass and about 3.5×2.5×1.8 cm at the intrascrotal mass. Some lumps had invaded the penile root without penile deviation and without pain on erection. There were no enlarged inguinal nodes. The laboratory results, including complete blood counts, serum electrolytes, testicular tumor markers, and urinalysis, were within the normal range. Scrotal ultrasonography revealed intrascrotal and extratesticular masses in the mid-scrotal region (Fig. 2). Complete excision of the scrotal masses was performed. After surgery, there was no testicular invasion. The mass was firm and appeared to be grossly homogeneous. Immunohistochemically, the tumor cells were positive to S-100 and negative to SMA (Fig. 1B). The pathologic diagnosis was schwannoma of the scrotum. There was no evidence of recurrence during 6 years of follow-up.
DISCUSSION
Schwannomas can present in a patient as a solitary tumor or as part of a systemic disease that may involve the nervous system. In spite of the abundant sensitive innervation of the genitalia, schwannomas of the scrotum are very rarely reported.1,2 In cases that have been described, documentation of multiple schwannomas of the scrotum have been very rare. In fact, to the best of our knowledge, previous reports of scrotal schwannomas have all been solitary cases.1-3 The present case is a very rare report of an extratesticular and intrascrotal schwannoma associated with multiple lesions.
Although neurogenic tumors are generally encountered in young and middle-aged adults,4 the presentation age of male genital schwannomas seems to be variable, and includes a significant number of elderly patients.
The clinical and radiologic findings of male genital schwannoma are non-specific and the lesion may be misdiagnosed as another type of solid tumor. These tumors are usually asymptomatic until they are large enough to compress the neighboring structures and induce various secondary symptoms, such as pain, dysuria, prolonged voiding time, or urinary retention. The most common sign at presentation was a solitary, painless, and firm genital mass. Ultrasonography, computed tomography, or magnetic resonance imaging can be helpful in locating the site and delineating the mass.
Immunohistochemical analysis can also be used to define the histological origin of the tumor. In this case, positive immunostaining for the S100 protein coupled with a negative reaction to CD34 and smooth-muscle actin and desmin were required to confirm the diagnosis of schwannoma and to rule out other diagnostic possibilities.
Multiple schwannomas in the same individual suggest two types of underlying tumor predisposition syndromes: neurofibromatosis 2 and schwannomatosis. Both of these diseases include familial and non-familial cases.5
Patients with schwannomatosis are at increased risk for developing new schwannomas anywhere in the body although the long-term outcome of schwannomatosis is favorable. Therefore, a complete annual physical and neurological evaluation is recommended.6
The therapeutic principle for male genital schwannoma is similar to that for managing schwannoma elsewhere in the body. A conventional surgical approach with complete excision of the mass is the most advisable treatment.7 Therefore, we recommend simple enucleation of the mass. Malignant change in intrascrotal extratesticular schwannoma is very rare.8,9 In our case, there was no evidence of recurrence during a 6-year follow-up.

 XML Download
XML Download