

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abscess of the penis is a rare infectious condition. Corporeal infection or abscess has been described as a complication of trauma, intracavernous injection therapy, cavernosography or foreign bodies, or as an unusual presentation of gonorrhea or tuberculosis.1-3 Spontaneous abscess of the corpus cavernosum has also been reported.4-6
Among the causes of penile abscess, penile fracture is an uncommon urologic emergency. It refers to the rupture of the tunica albuginea of the corpus cavernosum during sexual intercourse. Immediate surgical repair of the ruptured tunica albuginea is widely accepted as the treatment of choice. However, conservative management of penile fracture might result in penile curvature, abscess or plaque, and significantly longer recovery times.
We report a case of neglected penile fracture after intracavernosal vasoactive drug injection and sexual activity in a patient with uncontrolled diabetes. The case was further complicated by development of a penile abscess. This patient was successfully treated by surgical drainage of the abscess and primary closure of the ruptured tunica albuginea.
CASE REPORT
A 51-year-old man was referred with complaints of a painful swollen mass on the proximal penile shaft. The swelling was complicated by severe pain and gradual penile detumescence without a snap-pop sound during sexual intercourse after intracavernosal injection 9 days earlier. No more erections were reported thereafter. In spite of antibiotics and pain medications from a private clinic for a week, painful penile swelling has gradually progressed. The patient had been on medications for diabetes mellitus and hypertension for about 10 years, and he had a history of self-injection of petroleum jelly into the penis over the previous 20 years. The patient denied any history suggestive of sexually transmitted diseases.
On physical examination, he was afebrile and hemodynamically stable. A 5 cm tender and swollen mass was palpable on the ventral aspect of the right proximal penile shaft (Fig. 1A). The phallus deviated to the left side because of the mass effect. The petroleum jelly infiltrated skin was confined to the distal penile shaft, circumferentially. The external urethral meatus showed no discharge. Both testes and epididymides were palpably normal, and the inguinal lymph nodes were not enlarged. A rectal examination was also unremarkable.
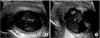
The random blood sugar (323 mg/dl) and white blood cell count (12,800/mm3) were elevated. Urine analysis and culture showed no evidence of infection. The serology for human immunodeficiency virus (HIV) and syphilis, and urine culture for tuberculosis were negative, as well. Penile ultrasonography showed an approximately 3.5 cm mixed echoic fluid collection along the right side of the penile shaft (Fig. 2).
Under spinal anesthesia, the thickened Buck's fascia over the penile abscess was incised, and about 10 ml of pus with a blood clot was drained (Fig. 1B). The culture of the abscess yielded Enterococcous faecalis. After irrigation with saline and povidone iodine inside of the abscess cavity, we found the ruptured tunica albuginea about 1 cm in length (Fig. 1C). However, the cavernosal tissue was intact without evidence of severe inflammatory change. The ruptured tunica albuginea was closed with Vicryl 4-0 interrupted sutures. The patient was discharged from the hospital on the day after surgery. During the follow up, superficial wound dehiscence occurred but healed after meticulous dressing and secondary wound closure.
DISCUSSION
Penile fracture is the disruption of the tunica albuginea with rupture of the corpus cavernosum. Fracture typically occurs during vigorous sexual intercourse, when the rigidly erect penis slips out of the vagina and strikes the perineum or pubic bone, sustaining a buckling injury. Patients usually describe a cracking or popping sound as the tunica tears, followed by pain, rapid detumescence, and discoloration and swelling of the penile shaft. If the Buck's fascia remains intact, the penile hematoma remains contained between the skin and tunica, resulting in a typical eggplant deformity. False fractures of the penis also have been reported, where both the corpora and tunica albuginea were found to be intact with no inflammatory change or curvature formation in spite of a definite suggestion of penile fracture and hematoma was noted within the Dartos fascia.2,7 The utility of imaging studies in the setting of the suspected penile fracture is controversial. Ultrasonography and magnetic resonance imaging have been recommended when the diagnosis is uncertain. Although our patient did not describe the classic 'snap-pop' or rapid detumescence during sexual intercourse that could explain penile fracture, we confirmed the rupture of the tunica albuginea of the right proximal corpus cavernosum on exploration.
On the other hand, penile abscesses are rare and can develop after trauma or penile prosthesis insertion, as a complication of intracavernosal injections, cavernosography or penile foreign body, or from undetermined causes.1-6 Predisposing factors include diabetes mellitus, HIV infection, or sexually transmitted disease. When Buck's fascia is penetrated by inflammation, there can be extensive necrosis of the subcutaneous tissue and fascia.2 The most common pathogen is Escherichia coli, followed by Neisseria gonorrhea with a previous history of sexually transmitted disease.8 The most plausible mechanism for the penile abscess of our patient was secondary infection of the penile hematoma as a result of neglected penile fracture. However, he had history of uncontrolled diabetes, intracavernosal injection therapy, and petroleum jelly infiltrated penile skin, which could be predisposed to infection. Therefore, patients who undergo intracavernosal injection therapy with any underlying conditions, such as diabetes, dental caries, or skin infections, should be cautioned about the possible development of penile abscess.
Patients with suspected penile fractures should be promptly explored and surgically repaired because conservative management can result in penile curvature, abscess or plaques, and significantly longer recovery times. In particular, penile abscess associated with penile fracture should be managed with surgical drainage and antibiotic therapy because it can be further complicated by the development of necrotizing fasciitis of the penile shaft.2 Therefore, abscess drainage, antibiotic therapy, and debridement are needed to complete excision of the sources of infection.
Our case indicates that penile abscess associated with penile fracture should be considered as a diagnosis in those who have undergone intracavernosal injection therapy or diabetes, and immediate surgical exploration is recommended in patients with suspected penile fracture.

 XML Download
XML Download