

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Malignant lymphoma of the bladder is a rare lesion, representing approximately 0.2% of primary neoplastic lesions and approximately 1.8% of secondary lesions.1 Patients with bladder lymphoma can be classified into 3 groups according to their clinical presentation: primary cases in the bladder, cases occurring in the bladder as a manifestation of systemic disease, and secondary cases with a clinical history of malignant lymphoma recurring in the bladder.2 Although urogenital involvement by malignant lymphoma has been demonstrated in approximately 7% of autopsies, a disseminated lymphoma clinically presenting as a bladder mass is a rare phonomenon.3 The authors report the case of a 71-year-old patient with concurrent bladder lymphoma and bladder urothelial carcinoma (UC) presenting as metastatic bladder UC. Bladder lymphoma in this patient was a manifestation of systemic disseminated disease.
CASE REPORT
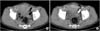
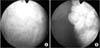
A 71-year-old man presented to our urologic department with a history of gross hematuria and dysuria for 1 month. Initial laboratory findings showed normochromic normocytic anemia without thrombocytopenia and an elevated level of lactate dehydrogenase at 798 IU/L. Abdominal computed tomography (CT) revealed a large bladder mass in the base and the left lateral wall of the bladder associated with perivesical infiltration and regional lymphadenopathy (Fig. 1). Abdominal CT also revealed a low attenuated, homogeneous mass in the distal ileum. Homogeneous, enlarged lymph nodes in the right pericardiophrenic angle, and around the suprahepatic inferior vena cava, aortocaval, right lower quadrant mesenteric, and bilateral inguinal areas were also seen. Cystoscopy revealed a large papillary mass in the trigone and left lateral wall of the bladder (Fig. 2). For histologic confirmation, the patient underwent transurethral resection of the bladder tumor. Histopathologic examination of specimens from the trigone specimen and the lateral wall confirmed superficial low-grade UC. In the subepithelial connective tissue, infiltration of atypical medium to large lymphocytes showing vesicular nuclei, prominent multiple nucleoli, and an appreciable amount of basophilic cytoplasm was seen (Fig. 3). For the stage work-up, positron emission tomography (PET), and ultrasonography-guided percutaneous biopsy of the right inguinal and axillary regions were performed, in addition to bone marrow biopsy bilaterally in the superior iliac crest. PET showed abnormal uptake in the bladder, small bowel mesentery, cervical spine, and the lymph nodes in the right pericardiophrenic angle, around the suprahepatic inferior vena cava, aortocaval, and both superior inguinal lesions. The right inguinal lymph node specimen showed a vague follicular growth pattern with relatively monotonous small lymphocytes, plasma cells, and plasmacytoid lymphocytes. They were positive for immunohistochemical stains for CD20, CD79a, Bcl-2, CD43, and immunoglobulin M (IgM). The VS38 immunohistochemical stain was positive (Fig. 4). Magnetic resonance imaging of the spine revealed an intradural mass at the 7th cervical level of the spine. Malignant lymphoma was found to be marginal zone B-cell lymphoma (MZBCL) based on the normal serum monoclonal IgM level and non-involvement of the bone marrow and spleen.
During preparation for chemotherapy, the patient underwent surgical exploration of the abdomen due to perforation of a lymphoma lesion in the distal ileum. At six months after transurethral resection of the bladder tumor, cystoscopy was performed for follow-up of the bladder tumor, which revealed a papillary tumor on the trigone and subsequent transurethral resection was conducted. The patient underwent 6 cycles of cyclophosphamide, doxorubicin, vincristine, and prednisolone chemotherapy but died from pneumonia and heart failure at 1 year after the end of chemotherapy.
DISCUSSION
Most tumors of the bladder are derived from the epithelium, and non-epithelial tumors are extremely rare.3 Metastatic tumors represent approximately 15% of all known bladder malignancies.4 In our case, the tumors of the bladder were demonstrated to be UC involving the epithelium and as B cell lymphoma in a subepithelial lesion. This is the first case of concurrent bladder tumors involving two different malignancies.
Usually, the diagnosis of bladder lymphoma is one of exclusion. It is made in the absence of any other nodal or extranodal involvement after biopsy with immunohistochemical study, and after a negative study of disease extension, which includes bone marrow biopsy and CT.4 This approach is changing with the introduction of PET to search for other nodal or extranodal involvement.
The most frequent symptoms of bladder lymphoma are gross hematuria followed by concomitant urinary tract infection, dysuria, and other lower urinary tract symptoms.4 The cystoscopic appearance of bladder lymphoma is a large, multinodular mass which has a characteristic submucosal pattern with minimal or no ulceration.5 The CT appearances of bladder lymphoma are multinodular thickening of the bladder wall, a lobulated mass involving the bladder wall, and intermittent extravesical extension.6
In our case, the cystoscopic appearance was a multiple papillary mass, which is a typical finding of bladder UC, and the CT showed multinodular thickening with extravesical extension and regional lymph node enlargement. Our first impression after cystoscopy and CT was metastatic bladder cancer with regional lymph node and small intestine metastasis. However, by comparing the CT findings of the bladder mass with other reported cases, it became clear that the multinodular pattern was a classic finding of bladder lymphoma.
MZBCL, previously known as monocytoid B-cell lymphoma in the lymph nodes, has been an evolving concept since these neoplasms were first described in the 1980s. It was only in the World Health Organization classification that extranodal, nodal, and splenic types of MZBCL became recognized as three distinct entities. Lymphoplasmacytic lymphoma (LPL) is characterized by a monoclonal expansion of predominantly small B-lymphocytes with variable plasmacytoid differentiation; small B-lymphocytes are usually CD5-, CD10-, and CD23-, and they are associated with serum IgM paraprotein.7 Although LPL is an indolent tumor in most cases, it also involves extramedullary sites. Lin et al8 reported 44 patients with LPL involving extramedullary sites, and LPL was subclassifed into lymphoplasmacytic, lymphoplasmacytioid, polymorphous, DLBCL transformed from LPL, and MZBCL. This subclassification in LPL with extranodal involvement suggested the possibility that these tumors are part of the spectrum of LPL. MZBCL is indistinguishable from LPL by histologic appearance and only distinguishable by elevation of serum monoclonal IgM and the involvement of the bone marrow.7
In conclusion, we describe an extremely infrequent instance of concurrent bladder tumors, which were demonstrated to be UC and MZBCL. Although the incidence of bladder lymphoma is low, in cases with gross hematuria, regional lymph node enlargement, and a multinodular pattern with bladder wall thickening in abdominal CT findings, the diagnosis of bladder lymphoma should be considered.


 XML Download
XML Download