

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Tuberculous prostatic abscess has been rarely reported.1 Intravesical bacillus Calmette-Guérin (BCG) has been a commonly-used therapy for non-muscle invasive urothelial carcinoma of the bladder since it was first introduced by Morales et al2 in 1976. This therapy may be complicated by granulomatous inflammatory disease within the urinary tract. Tubercular prostatic abscess is one possible complication.3,4
We report a case of tuberculous prostatitis with abscess found during a postoperative follow-up evaluation of bladder cancer.
CASE REPORT
A 56-year-old man visited the Department of Urology for hematuria. A cystoscopic examination was performed and a bladder mass was found. He underwent a transurethral resection of a bladder tumor (TURBT) for a low grade T1 urothelial carcinoma. He had been treated for pulmonary tuberculosis with an anti-tuberculous agent for 6 months approximately 14 years earlier. The chest X-ray at the time of the initial visit showed an inactive pulmonary tuberculosis lesion in the right apical lung. Intravesical BCG (OncoTice®, Organon Teknika, Boxtel, Netherlands) instillations were performed once per week for 6 weeks at a concentration of 12.5 mg in 50 ml saline.
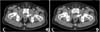
Six months after TURBT following the completion of induction BCG therapy, the patient complained of frequency, dysuria, and perineal discomfort. A digital rectal examination (DRE) showed tenderness in the right lobe of the prostate. A computed tomography (CT) scan was performed for the evaluation of prostate infection and revealed an oval-shaped low density lesion (Fig. 1A). The level of prostate specific antigen, which had been 0.2 ng/ml 6 months earlier, was 2.17 ng/ml. For the differential diagnosis of the prostatic oval-shaped low density lesion, a prostate biopsy was performed. The histology of the needle biopsy showed granulomatous inflammation of the prostate with caseating necrosis in the prostate specimens. A Ziehl-Neelsen stain revealed a few acid-fast bacilli (Fig. 2). The tuberculous prostatic abscess was confirmed. The patient was treated with a 12 month anti-tuberculous regimen of isoniazid (300 mg), rifampicin (600 mg), ethambutol (800 mg), and pyrazinamide (1,500 mg) daily. The follow-up CT showed the disappearance of the prostatic abscess (Fig. 1B) after 12 months of anti-tuberculous medication.
DISCUSSION
In this case, an oval-shaped low density lesion at the prostate that was confirmed as a tuberculous prostate abscess was found in a postoperative follow-up evaluation of bladder cancer. Patients with tuberous prostatic abscess have been treated by transperineal drainage with a 9- or 12-month regimen of anti-tuberculosis drugs.3,4 Because the size of the prostate abscess was small in this patient, drainage was not performed. The patient was treated with anti-tuberculous medications (isoniazid (300 mg), rifampicin (600 mg), ethambutol (800 mg), and pyrazinamide (1,500 mg) daily). A follow-up CT showed the disappearance of the prostatic abscess (Fig. 1B) after 12 months of treatment with anti-tuberculous medications.
With the increasing use of intravesical BCG therapy in non-muscle invasive bladder cancer, tubercular infection of the prostate is likely to increase. The route of infection of tuberculosis in the prostate is mainly through the hematogenous spread and direct extension of infection.5 In this patient, tuberculous prostatitis with abscess after intravesical BCG therapy may be through the direct extension of tuberculosis from the bladder. If the diagnosis and treatment of a prostate abscess is delayed, it can progress to sepsis. Therefore, proper diagnosis and treatment is important. Diagnosis of a prostate abscess is performed using transrectal ultrasonography or a CT scan and it is treated by drainage or anti-tuberculosis drugs.3,4 If DRE shows a palpable prostate mass in older patients, a prostate biopsy is necessary for the differential diagnosis of prostate cancer.5 In this patient, the histology of the biopsy showed tuberculous prostatitis. This case illustrates that when BCG immunotherapy for bladder cancer is performed, tuberculous prostatitis with abscess can develop.

 XML Download
XML Download