

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nocturia is one of the common lower urinary tract symptoms (LUTS), the third most bothersome symptom in all subject and the most bothersome symptom in men with benign prostatic hyperplasia (BPH).1-4 This symptom is often associated with bladder outlet obstruction and with impairing health related quality of life (QoL).4,5 Nocturia is defined as waking at night one or more times to void.6 Evaluating the impact of nocturia on sleep quality in patients with LUTS is needed.
Although the International Prostate Symptom Score (IPSS) is commonly used, it does not show how strongly nocturia decreases sleep quality.7 The Pittsburgh Sleep Quality Index (PSQI) is a questionnaire related to the sleep quality used worldwide.8,9 This study was performed to evaluate that how strongly nocturia impacts sleep quality evaluated by PQSI in patients with LUTS/BPH.
MATERIALS AND METHODS
Men with LUTS/BPH who visited a hospital's Department of Urologybetween January and December 2010 were selected for the study. Approval for this study was obtained from the Institutional Review Board at the hospital and informed consent was obtained from each patient. Patients were included in the study if they met the criteria of the 5th International Consensus Committee on BPH (Paris, 2000), voided more than 150 ml during uroflowmetry, and were measured postvoid residual urine (PVR) volume and prostate size. Patients who reported more than one episode of nocturia per night using question 7 of the IPSS, had a maximum urinary flow rate (Qmax) under 15 ml/sec, a total IPSS over 7, a digital rectal examination negative for suspected malignancy, and a prostate volume larger than 20 ml were assessed as being in the LUTS/BPH group. LUTS/BPH patients without nocturia were included in the control group. The exclusion criteria included the use of diuretics for treating congestive heart failure, the use of sedatives or tranquilizers for treating sleep disturbances, or having neurogenic bladder dysfunction. Patients were also excluded from the analysis if they had a documented history or clinical symptoms of prostatitis, prostate cancer, a history of prostate surgery or radiotherapy, or acute urinary retention. The quality of sleep was measured using the PSQI. The overall score can range from 0 (absence of sleep-related problems) to 21 (severe sleep-related problems). A total score of >5 is considered an indicator of severe sleep disorders.8 Prostate volume was measured by transrectal ultrasonography. Data are expressed as mean±standard error and compared statistically using the Student's t-test, chi-squared test, and Pearson correlation test. A level of p<0.05 was considered statistically significant.
RESULTS
1. Profiles
Seven patients without nocturia (41.2%) had associated diseases, including 1 (5.9%) with hypertension, 4 (23.5%) with diabetes, 1 (5.9%) with herniated intervertebral disk, and 1 (5.9%) with hypothyroidism. Thirty two patients with nocturia (55.2%) had associated diseases, including 14 (24.1%) with hypertension, 11 (19.0%) with diabetes, and 7 (12.1%) with hyperlipidemia. A total of 75 male patients (17 without and 58 patients with nocturia) with LUTS/BPH were enrolled. 58 patients with nocturia had one or more episodes of nocturia: one (11 patients), two (15 patients), three (15 patients), four (11 patients), and five (6 patients) episodes. Baseline mean age, prostate volume, and prostate specific antigren (PSA) levels did not differ between patients with or without nocturia (Table 1).
2. Uroflowmetry
The baseline mean Qmax of the patients without and with nocturia were 12.0±1.0 and 11.2±0.8, respectively. The baseline mean PVR volume of the patients without and with nocturia were 10.9±5.8 and 19.2±0.8, respectively. There was no significant difference in Qmax or PVR volume between patients without or with nocturia (p>0.05, Table 1).
3. IPSS
The mean number of episodes of nocturia using question 7 of the IPSS was 2.8±0.2. The mean total IPSS of the patients without and with nocturia was 12.94±6.04 and 15.0±0.7, respectively. The mean QoL index of the patients without and with nocturia was 2.82±1.2 and 3.4±0.1, respectively. The mean total IPSS and QoL index of patients with nocturia were higher than those of patients without nocturia (p<0.05, Table 1).
4. Sleep quality
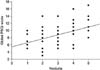
The patients with nocturia showed a higher mean global PSQI (8.5±0.4) than the patients without nocturia (4.82±0.4). (p<0.01, Fig. 1). The patients with nocturia showed a higher percentage of severe sleep disorders (74.1%) than the patients without nocturia (35.3%, Fig. 2) (p<0.01). The patients with nocturia showed a lower subjective sleep quality, habitual sleep efficiency, sleep disturbances, and daytime dysfunction than patients without nocturia (Table 2). The regression coefficient between number of nocturia and mean global PSQI was 0.42 (p<0.01, Fig. 3).
DISCUSSION
The incidence of nocturia has been reported at a frequency of 16% in men aged 40~49 years, to 60% in men aged 70~79 years.10,11 In many cases nocturia may be caused by BPH.12
Poor sleep quality due to nocturia increased daytime fatigue and lowered levels of general well-being.10 Moreover, nocturia can be a risk factor for falling.13,14 The decrease in a patient's QoL due to nocturia represents a social and economic problem,15 and a higher prevalence of cardiovascular diseases was reported in men with nocturia.16
In this study, there was no significant difference in age, prostate volume, PSA, QMax, or PVR between patients without or with nocturia. The mean total IPSS scores and QoL index of patients with nocturia were higher than those of patients without nocturia.
The IPSS and QoL index are questionnaires used worldwide in relation to LUTS/BPH. Nocturia also has a severe impact on a patient's sleep quality because it causes a condition of worry about the need to wake to urinate. However, the IPSS and QoL index do not show how strongly nocturia decreases sleep quality.7 The PSQI is a simple, self administered questionnaire that contains 19 items assessing a wide variety of factors related to sleep quality.8,9 Global PSQI scores over 5 are considered to be an indicator of severe sleep disorders.8 In this study, patients with nocturia showed a higher mean global PSQI than patients without nocturia. Patients with nocturia also showed a higher percentage of severe sleep disorders, subjective sleep quality, habitual sleep efficiency, sleep disturbances, and daytime dysfunction than patients without nocturia. The regression coefficient between the number of episodes of nocturia and the mean global PSQI was significant. Therefore, nocturia has strong impact on sleep quality in patients with LUTS/BPH.




 XML Download
XML Download